

This is a preprint.
Prevalence of Olfactory Dysfunction with the Omicron Variant of SARS-CoV-2: A Systematic Review and Meta-analysis
- PMID: 36561176
- PMCID: PMC9774228
- DOI: 10.1101/2022.12.16.22283582
Prevalence of Olfactory Dysfunction with the Omicron Variant of SARS-CoV-2: A Systematic Review and Meta-analysis
Update in
-
Prevalence of Olfactory Dysfunction with the Omicron Variant of SARS-CoV-2: A Systematic Review and Meta-Analysis.Cells. 2023 Jan 28;12(3):430. doi: 10.3390/cells12030430. Cells. 2023. PMID: 36766771 Free PMC article.
Abstract
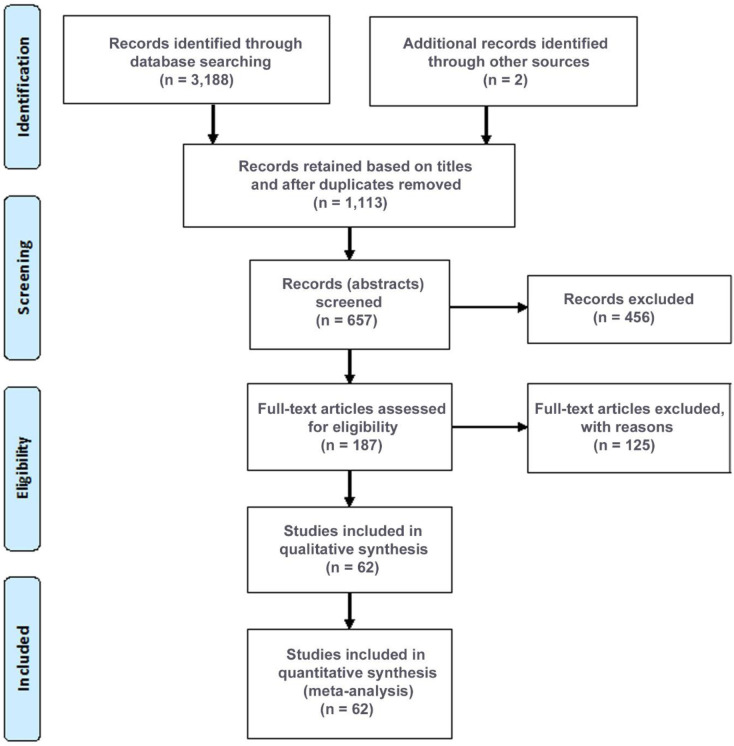
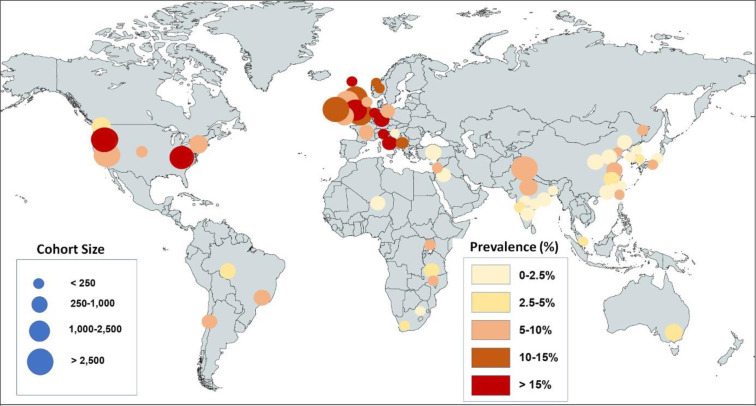
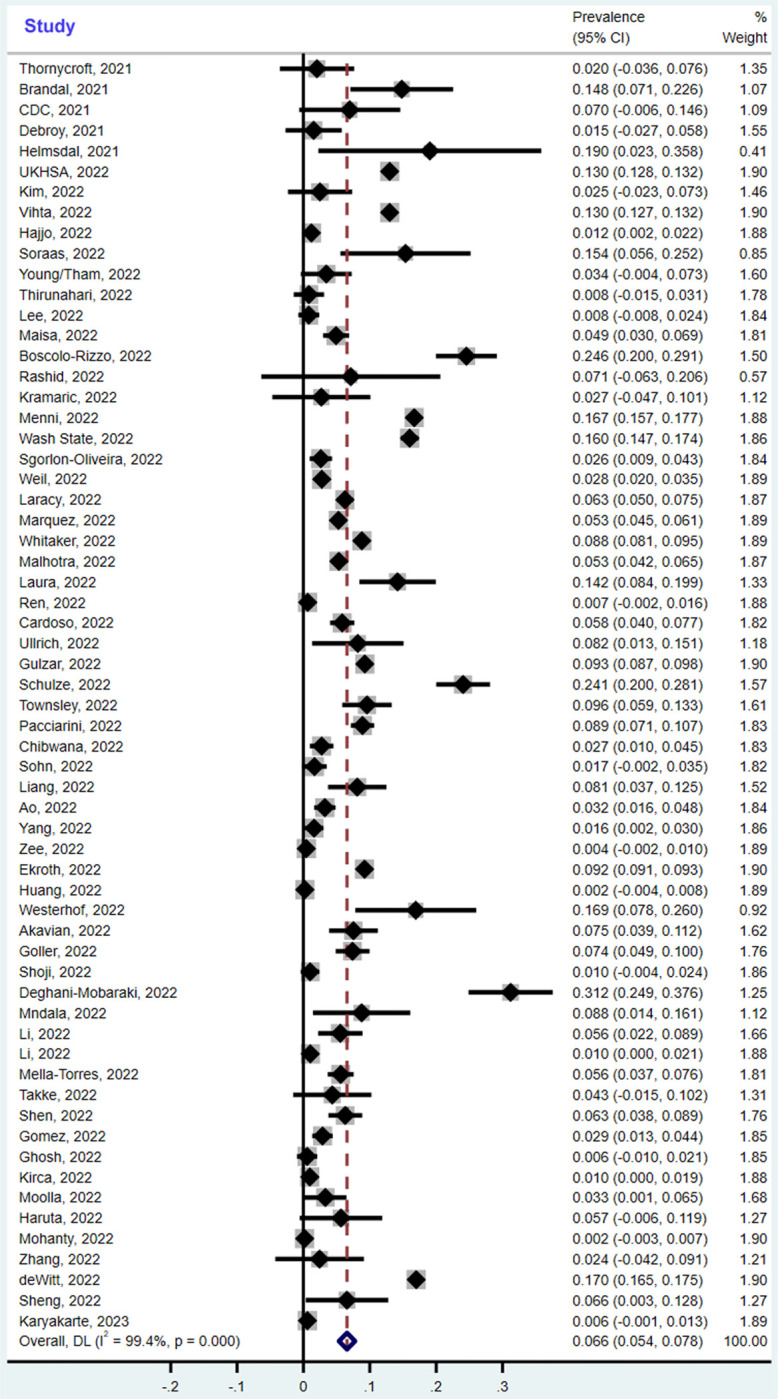
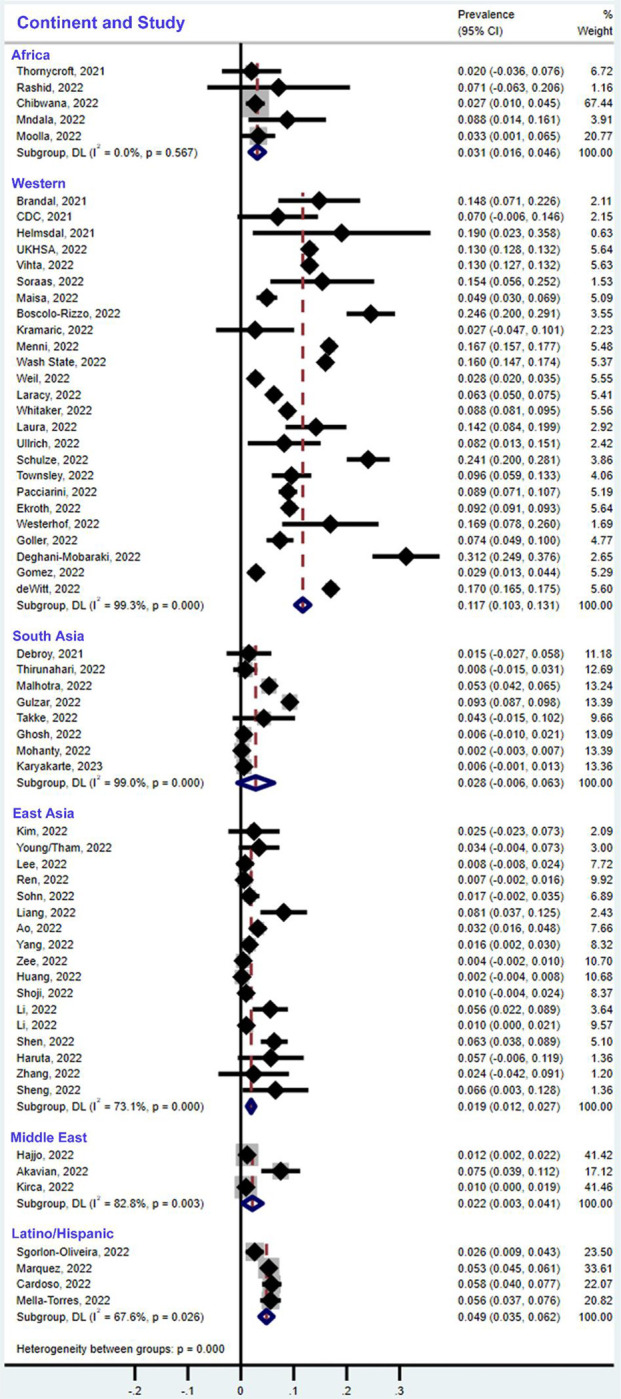
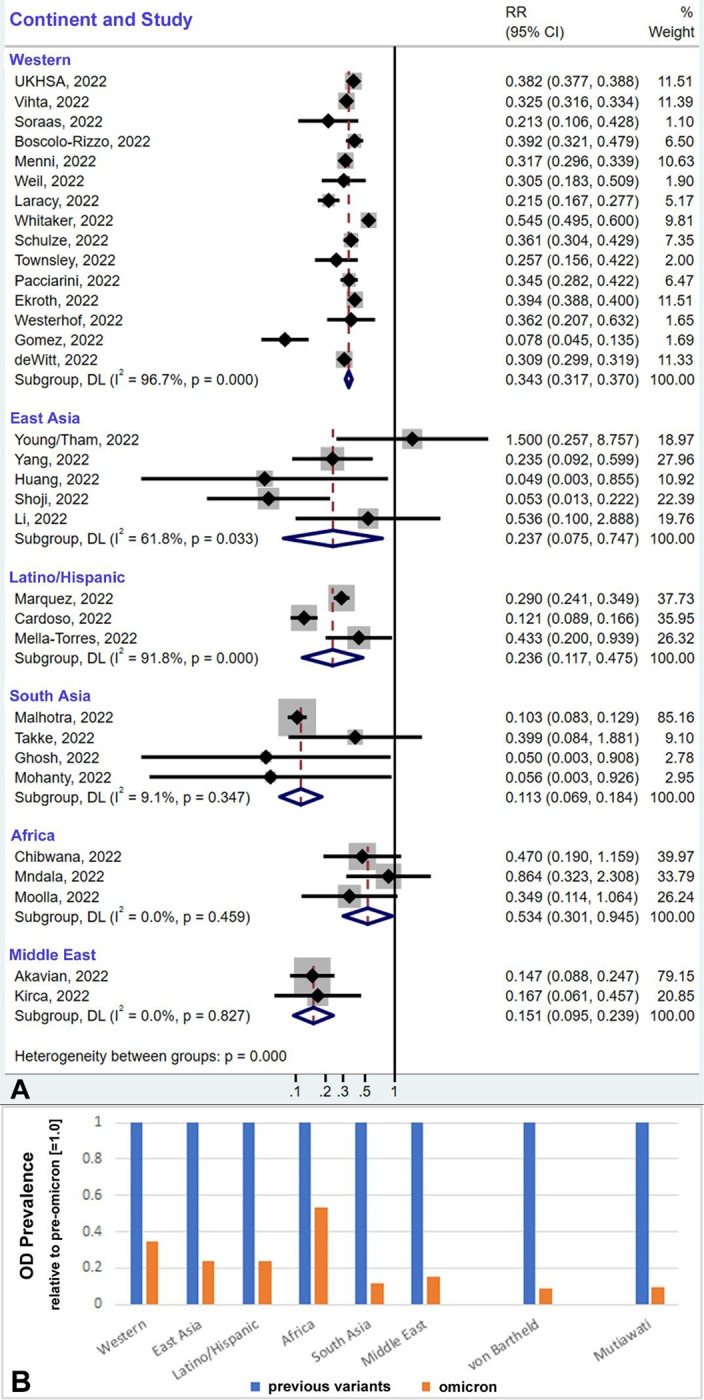
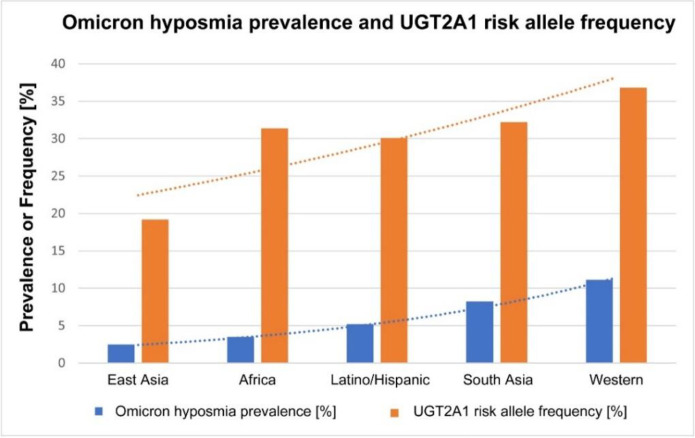
The omicron variant is thought to cause less olfactory dysfunction than previous variants of SARS-CoV-2, but the reported prevalence differs greatly between populations and studies. Our systematic review and meta-analysis provide information about regional differences in prevalence as well as an estimate of the global prevalence of olfactory dysfunction based on 62 studies reporting on 626,035 patients infected with the omicron variant. Our estimate of the omicron-induced prevalence of olfactory dysfunction in populations of European ancestry is 11.7%, while it is significantly lower in all other populations, ranging between 1.9% and 4.9%. When ethnic differences and population sizes are taken into account, the global prevalence of omicron-induced olfactory dysfunction in adults is estimated at 3.7%. Omicron’s effect on olfaction is twofold to tenfold lower than that of the alpha or delta variant, according to previous meta-analyses and our analysis of studies that directly compared prevalence of olfactory dysfunction between omicron and previous variants. The profile of prevalence differences between ethnicities mirrors the results of a recent genome-wide association study that implicated a gene locus encoding an odorant-metabolizing enzyme, UDP glycosyltransferase, to be linked to the extent of COVID-related loss of smell. Our analysis is consistent with the hypothesis that this enzyme contributes to the observed population differences.
Conflict of interest statement
Conflict of interest
The authors declare no conflict of interest.
Figures
References
-
- Patt Y.S.; David P.; Bergwerk M.; Shoenfeld Y. The Reduced Frequency of Olfactory Dysfunction in Patients with Omicron SARS-CoV-2 Variant Infection. Ann. Otolaryngol. Rhinol. 2022, 9, 1302.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous