

Accuracy of non-gated low-dose non-contrast chest CT with tin filtration for coronary artery calcium scoring
- PMID: 36561207
- PMCID: PMC9764023
- DOI: 10.1016/j.ejro.2022.100396
Accuracy of non-gated low-dose non-contrast chest CT with tin filtration for coronary artery calcium scoring
Abstract
Objective: The study investigated the accuracy of coronary artery calcium scores (CACS) and the potential for reducing radiation dose using non-gated low-dose non-contrast chest computed tomography (CT) scanning with tin filtration for one-stop screening of the lungs and heart.
Methods: A prospective study was conducted,193 Patients received two scans for determining CACS, including an ECG-gated CT at 120 kV (ECG-gated CT), followed by a non-gated low-dose chest CT using 100 kV with tin filtration (non-gated Sn100 kV-LDCT). The Agatston score (AS), risk stratification, and radiation dose were compared between the scan types.
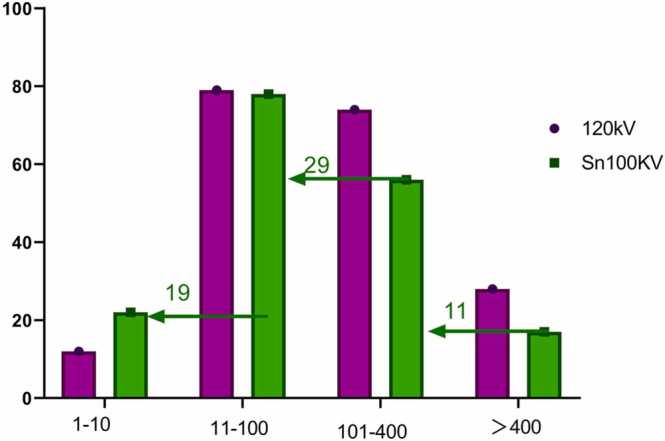
Results: There was good consistency in the AS from both an ECG-gated CT and a non-gated low-dose chest CT scan, which had a high correlation (r = 0.970). The Kappa value of risk stratification of the two scan types was 0.549. The area under the ROC curve (AUC) of the CACS was used to develop a new risk stratification standard for non-gated Sn100 kV-LDCT evaluation of CACS. In comparison to the CACS measured by ECG-gated CT, non-gated Sn100 kV-LDCT had an AUC of 0.951 and an optimal critical value of 4.6 in the low-risk category. The AUC of low-medium risk was 0.966, and the optimal critical value was 41.2. The AUC of the medium-high risk category was 0.968, and the optimal critical value was 230. The consistency in CACS measured by ECG-gated CT and non-gated Sn100 kV-LDCT had a Kappa value of 0.831. The Effective dose (ED) of non-gated Sn100 kV-LDCT and ECG-gated CT was 0.056 ± 0.017 mSv and 0.685 ± 0.455 mSv, respectively (p < 0.05).
Conclusion: The Agatston score of CACS using non-gated low-dose chest CT was accurate, but there was an underestimation in risk stratification. This study developed a new risk stratification standard for non-gated Sn100 kV-LDCT evaluation of CACS, which is in closer agreement with CACS derived from ECG-gated CT scans.
Keywords: Chest; Computed tomography; Coronary Artery Calcium Scoring; Low dose; Tin Filtration.
© 2022 The Authors. Published by Elsevier Ltd.
Figures





Similar articles
-
Performance of fully automated deep-learning-based coronary artery calcium scoring in ECG-gated calcium CT and non-gated low-dose chest CT.Eur Radiol. 2025 May 10. doi: 10.1007/s00330-025-11559-4. Online ahead of print. Eur Radiol. 2025. PMID: 40348882
-
Accuracy and Radiation Dose Reduction Using Low-Voltage Computed Tomography Coronary Artery Calcium Scoring With Tin Filtration.Am J Cardiol. 2017 Feb 15;119(4):675-680. doi: 10.1016/j.amjcard.2016.10.051. Epub 2016 Nov 16. Am J Cardiol. 2017. PMID: 27986261
-
Feasibility analysis of non-electrocardiogram-triggered chest low-dose computed tomography using a kV-independent reconstruction algorithm for predicting cardiovascular disease risk in patients receiving maintenance hemodialysis.BMC Cardiovasc Disord. 2025 Jan 24;25(1):48. doi: 10.1186/s12872-025-04499-w. BMC Cardiovasc Disord. 2025. PMID: 39849362 Free PMC article.
-
The Future of Concurrent Automated Coronary Artery Calcium Scoring on Screening Low-Dose Computed Tomography.Cureus. 2020 Jun 12;12(6):e8574. doi: 10.7759/cureus.8574. Cureus. 2020. PMID: 32670710 Free PMC article. Review.
-
Current status and future perspective of coronary artery calcium score in asymptomatic individuals.J Cardiol. 2025 Apr;85(4):275-282. doi: 10.1016/j.jjcc.2024.11.008. Epub 2024 Dec 2. J Cardiol. 2025. PMID: 39631694 Review.
Cited by
-
Performance assessment of an artificial intelligence-based coronary artery calcium scoring algorithm in non-gated chest CT scans of different slice thickness.Quant Imaging Med Surg. 2024 Aug 1;14(8):5708-5720. doi: 10.21037/qims-24-247. Epub 2024 Jul 24. Quant Imaging Med Surg. 2024. PMID: 39144022 Free PMC article.
-
Exploring the interplay between epicardial fat, coronary artery calcium score, and nonalcoholic fatty liver disease through non-ECG-gated chest computed tomography: A cross-sectional study.Health Sci Rep. 2024 Aug 20;7(8):e70010. doi: 10.1002/hsr2.70010. eCollection 2024 Aug. Health Sci Rep. 2024. PMID: 39170884 Free PMC article.
-
Evaluation of low-dose chest scans for coronary artery calcium scoring using photon-counting computed tomography with different slice thicknesses and iterative reconstruction levels.Quant Imaging Med Surg. 2025 Apr 1;15(4):3565-3574. doi: 10.21037/qims-24-1244. Epub 2025 Mar 25. Quant Imaging Med Surg. 2025. PMID: 40242329 Free PMC article.
-
Prevalence and clinical implications of coronary artery calcium scoring on non-gated thoracic computed tomography: a systematic review and meta-analysis.Eur Radiol. 2024 Jul;34(7):4459-4474. doi: 10.1007/s00330-023-10439-z. Epub 2023 Dec 22. Eur Radiol. 2024. PMID: 38133672 Free PMC article.
-
Updates on CAD risk assessment: using the coronary artery calcium score in combination with traditional risk factors.Egypt Heart J. 2025 Jan 23;77(1):14. doi: 10.1186/s43044-025-00608-4. Egypt Heart J. 2025. PMID: 39847250 Free PMC article. Review.
References
-
- Hecht H.S. Coronary artery calcium scanning:past,present,and future. JACC Cardiovasc. Imaging. 2015;8:579–596. - PubMed
-
- Erbel R., Möhlenkamp S., Moebus S., Schmermund A., Lehmann N., Stang A., Dragano N., Grönemeyer D., Seibel R., Kälsch H., Bröcker-Preuss M., Mann K., Siegrist J., Jöckel K.H., Heinz Nixdorf Recall Study Investigative G. Coronary risk stratification, discrimination, and reclassification improvement based on quantification of Subclinical coronary atherosclerosis: the Heinz Nixdorf recall study. J. Am. Coll. Cardiol. 2010;56(17):1397–1406. - PubMed
-
- Silverman M.G., Blaha M.J., Krumholz H.M., Budoff M.J., Blankstein R., Sibley C.T., Agatston A., Blumenthal R.S., Nasir K. Impact of coronary artery calcium on coronary heart disease events in individuals at the extremes of traditional risk factor burden: the multi-ethnic study of atherosclerosis. Eur. Heart J. 2014;35(33):2232–2241. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
