

Approach to Complex Lower Extremity Reconstruction
- PMID: 36561427
- PMCID: PMC9762997
- DOI: 10.1055/s-0042-1758205
Approach to Complex Lower Extremity Reconstruction
Abstract
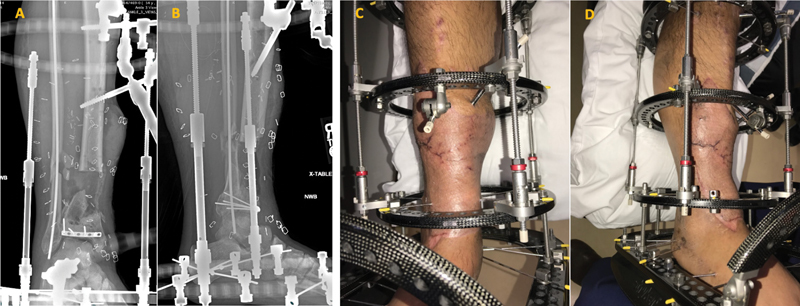
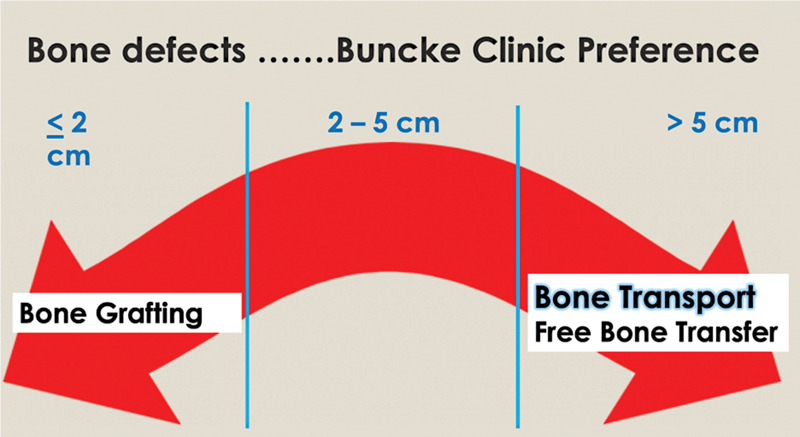
Composite injuries to the lower extremity from etiologies including trauma and infection present a complex dilemma for the reconstructive surgeon, and require multidisciplinary collaboration amongst plastic, vascular, and orthopaedic surgical specialties. Here we present our algorithm for lower-extremity reconstructive management, refined over the last decades to provide an optimized outcome for our patients. Reconstruction is predicated on the establishment of a clean and living wound, where quality of the wound-bed is prioritized over timing to soft-tissue coverage. Once established, soft-tissues and fractures are provisionally stabilized; our preference for definitive coverage is for microvascular free-tissue, due to the paucity of healthy soft-tissue available at the injury, and ability to avoid the zone of injury for microvascular anastomosis. Finally, definitive bony reconstruction is dictated by the length and location of long-bone defect, with a preference to utilize bone transport for defects longer than 5 cm.
Keywords: fractures; lower extremity; negative pressure wound therapy.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures






References
-
- Nance M L. 2012 National Trauma Data Bank Annual Report. American College of Surgeons. 2012:146.
-
- Georgiadis G M, Behrens F F, Joyce M J, Earle A S, Simmons A L. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. J Bone Joint Surg Am. 1993;75(10):1431–1441. - PubMed
-
- Lowenberg D W, Buntic R F, Buncke G M, Parrett B M. Long-term results and costs of muscle flap coverage with Ilizarov bone transport in lower limb salvage. J Orthop Trauma. 2013;27(10):576–581. - PubMed
-
- Bosse M J, MacKenzie E J, Kellam J F. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002;347(24):1924–1931. - PubMed
-
- Laughlin R T, Smith K L, Russell R C, Hayes J M. Late functional outcome in patients with tibia fractures covered with free muscle flaps. J Orthop Trauma. 1993;7(02):123–129. - PubMed
