

Theoretical Schemas to Guide Back Pain Consortium (BACPAC) Chronic Low Back Pain Clinical Research
- PMID: 36562563
- PMCID: PMC10403312
- DOI: 10.1093/pm/pnac196
Theoretical Schemas to Guide Back Pain Consortium (BACPAC) Chronic Low Back Pain Clinical Research
Abstract
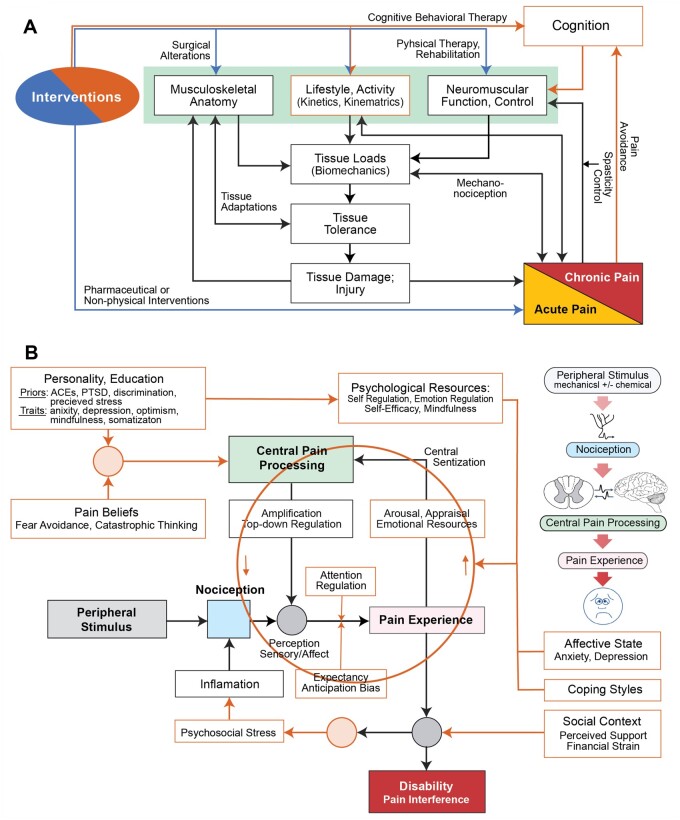
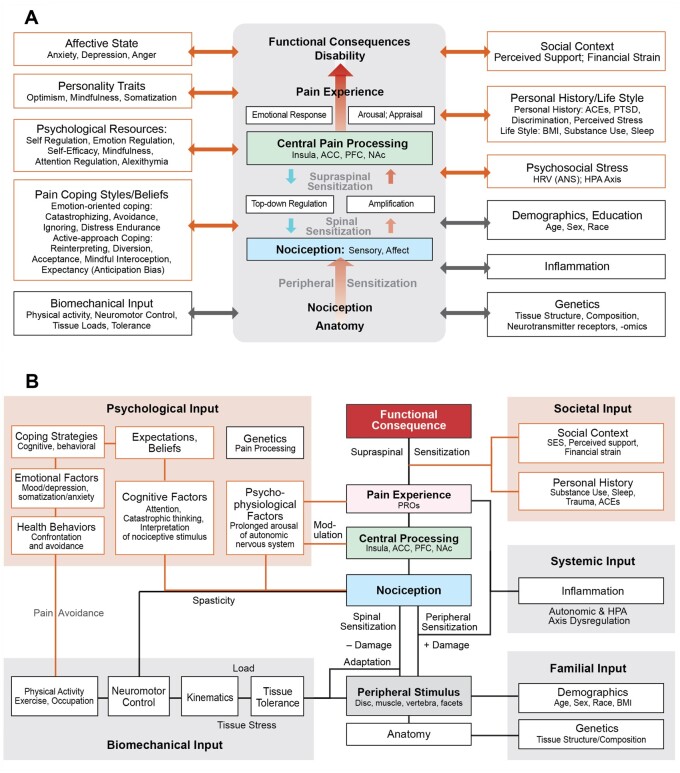
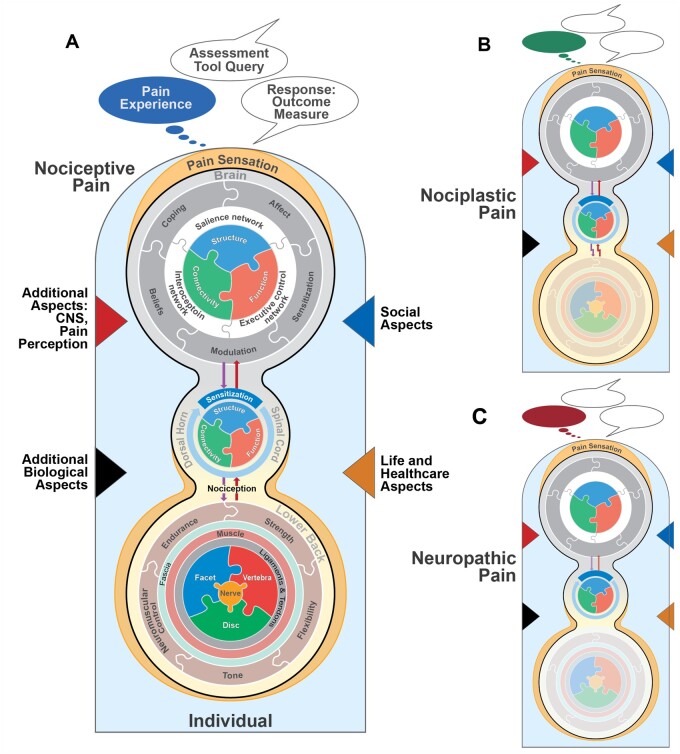
Background: Chronic low back pain (cLBP) is a complex with a heterogenous clinical presentation. A better understanding of the factors that contribute to cLBP is needed for accurate diagnosis, optimal treatment, and identification of mechanistic targets for new therapies. The Back Pain Consortium (BACPAC) Research Program provides a unique opportunity in this regard, as it will generate large clinical datasets, including a diverse set of harmonized measurements. The Theoretical Model Working Group was established to guide BACPAC research and to organize new knowledge within a mechanistic framework. This article summarizes the initial work of the Theoretical Model Working Group. It includes a three-stage integration of expert opinion and an umbrella literature review of factors that affect cLBP severity and chronicity.
Methods: During Stage 1, experts from across BACPAC established a taxonomy for risk and prognostic factors (RPFs) and preliminary graphical depictions. During Stage 2, a separate team conducted a literature review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to establish working definitions, associated data elements, and overall strength of evidence for identified RPFs. These were subsequently integrated with expert opinion during Stage 3.
Results: The majority (∼80%) of RPFs had little strength-of-evidence confidence, whereas seven factors had substantial confidence for either a positive association with cLBP (pain-related anxiety, serum C-reactive protein, diabetes, and anticipatory/compensatory postural adjustments) or no association with cLBP (serum interleukin 1-beta / interleukin 6, transversus muscle morphology/activity, and quantitative sensory testing).
Conclusion: This theoretical perspective will evolve over time as BACPAC investigators link empirical results to theory, challenge current ideas of the biopsychosocial model, and use a systems approach to develop tools and algorithms that disentangle the dynamic interactions among cLBP factors.
Keywords: Chronic Pain; Low Back Pain; Measurement; Research; Spine; Theoretical Model.
© The Author(s) 2022. Published by Oxford University Press on behalf of the American Academy of Pain Medicine.
Figures
References
-
- Corns J. Recent work on pain. Anal Rev 2018;78(4):737–53.
-
- Maher C, Underwood M, Buchbinder R.. Non-specific low back pain. Lancet 2017;389(10070):736–47. - PubMed
-
- Hartvigsen J, Hancock MJ, Kongsted A, et al. ; Lancet Low Back Pain Series Working Group. What low back pain is and why we need to pay attention. Lancet 2018;391(10137):2356–67. - PubMed
