

Safety and activity of anti-mesothelin antibody-drug conjugate anetumab ravtansine in combination with pegylated-liposomal doxorubicin in platinum-resistant ovarian cancer: multicenter, phase Ib dose escalation and expansion study
- PMID: 36564099
- PMCID: PMC10086500
- DOI: 10.1136/ijgc-2022-003927
Safety and activity of anti-mesothelin antibody-drug conjugate anetumab ravtansine in combination with pegylated-liposomal doxorubicin in platinum-resistant ovarian cancer: multicenter, phase Ib dose escalation and expansion study
Abstract
Objectives: Anetumab ravtansine is an antibody-drug conjugate consisting of a fully human anti-mesothelin monoclonal antibody conjugated to cytotoxic maytansinoid tubulin inhibitor DM4. Mesothelin is highly expressed in ovarian cancer. This phase Ib study determines the safety, pharmacokinetics, and anti-tumor activity of anetumab ravtansine and pegylated liposomal doxorubicin in mesothelin-expressing platinum-resistant ovarian cancer.
Methods: Anetumab ravtansine (5.5 or 6.5 mg/kg) and pegylated liposomal doxorubicin (30 mg/m2) were administered intravenously every 3 weeks to 65 patients with platinum-resistant epithelial ovarian cancer. Mesothelin expression was assessed by central immunohistochemistry. Adverse events, tumor response (RECIST 1.1), and progression-free survival were determined. Biomarker samples were assessed by ELISA and next-generation sequencing.
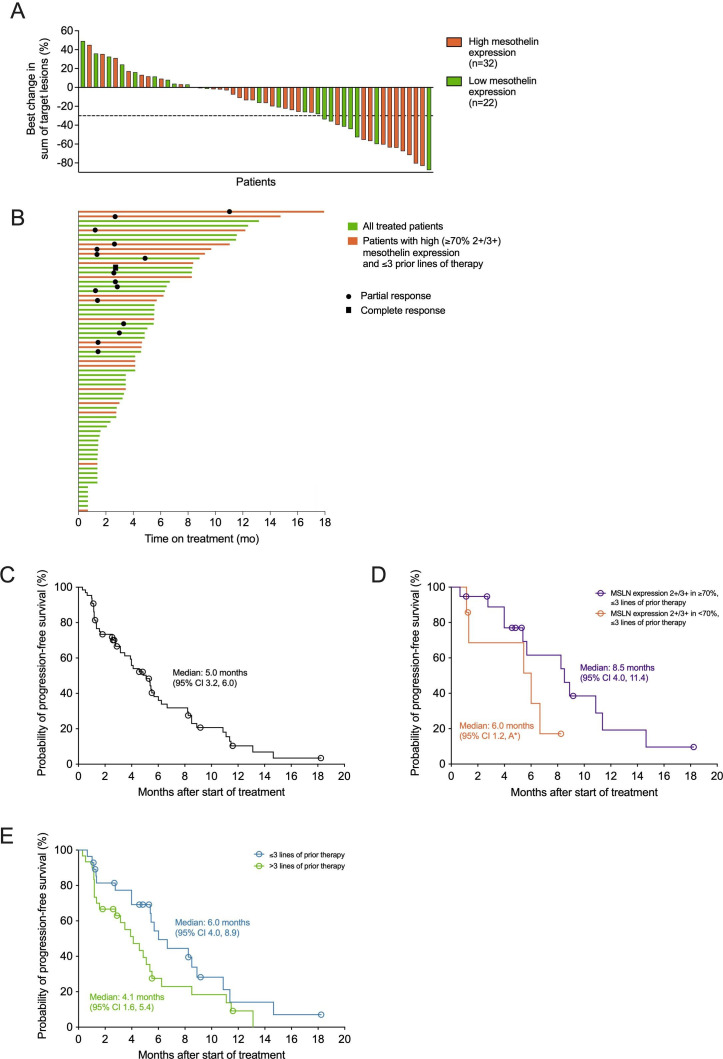
Results: In dose escalation, nine patients received anetumab ravtansine across two doses (5.5 or 6.5 mg/kg). The maximum tolerated dose of anetumab ravtansine was 6.5 mg/kg every 3 weeks and no dose-limiting toxicities were observed. In dose expansion, 56 patients were treated at the maximum tolerated dose. The most common treatment-emergent adverse events of any grade were nausea (47.7%), decreased appetite (43.1%), fatigue (38.5%), diarrhea (32.3%), and corneal disorder (29.2%). In all treated patients the objective response rate was 27.7% (95% CI 17.3% to 40.2%), including one complete (1.5%) and 17 partial responses (26.2%), with median duration of response of 7.6 (95% CI 3.3 to 10.2) months and median progression-free survival of 5.0 (95% CI 3.2 to 6.0) months. In an exploratory analysis of a sub-set of patients (n=19) with high mesothelin expression who received ≤3 prior lines of systemic therapy, the objective response rate was 42.1% (95% CI 20.3% to 66.5%) with a median duration of response of 8.3 (95% CI 4.1 to 12.0) months and median progression-free survival of 8.5 (95% CI 4.0 to 11.4) months.
Conclusions: Anetumab ravtansine and pegylated liposomal doxorubicin showed tolerability and promising clinical activity. These results established the dose schedule and the mesothelin-positive target population of this combination for a phase III study in platinum-resistant ovarian cancer.
Trial registration number: NCT02751918.
Keywords: ovarian cancer.
© IGCS and ESGO 2023. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: ADS: grants from Puma, Immunomedics, Gilead, Synthon, Boehringer-Ingelheim, and Genentech; grants and consulting fees from Merck, Tesaro, Eisai, and R-Pharma USA. IV reports the following conflicts of interest: consulting (2019–2021): Agenus (2021), Aksebio (2021), Amgen (Europe) (2019), AstraZeneca (2019–2022), Bristol Myers Squibb (2021), Clovis Oncology (2019), Carrick Therapeutics (2019), Deciphera Pharmaceuticals (2020–2021), Eisai (2021), Elevar Therapeutics (2020), F. Hoffmann-La Roche (2019–2021), Genmab (2019–2021), GSK (2019–2021), Immunogen (2019–2022), Jazzpharma (2021–2022), Karyopharm (2021), Mersana (2020), Millennium Pharmaceuticals (2019), MSD (2019–2022), Novocure (2020–2022), Novartis (2021), Octimet Oncology NV (2019), Oncoinvent AS (2019–2022), Sanofi (2021), Seagen (2021), Sotio a.s. (2019–2022), Verastem Oncology (2020), Zentalis (2020); contracted research for Oncoinvent AS (2019–2020) and Genmab (2019–2019); and grants (corporate sponsored research) from Amgen (2019–2020) and Roche (2019–2020). AGM: consulting work for Amgen, AstraZeneca, Clovis Oncology, Eisai, F. Hoffmann-La Roche, Genmab, GSK, Immunogen, Mersana, MSD, Novocure, Novartis, Oncoinvent, Seagen, and Sotio; speaker work for AstraZeneca, GSK, Clovis, and Roche; IST funding from Roche and GSK. KNM: advisory boards for AstraZeneca, Aravive, Alkemeres, Clovis, Eisai, EMD/Serono, GSK/Tesaro, Genentech/Roche, Hengrui, Immunogen, INxmed, IMAB, Lilly, Merck, Mereo, Mersana, Myriad, Novartis, OncXerna, OncoNova, Tarveda, Verastem, and VBL Therapeutics; research funding from PTC Therapeutics, Clovis, GSK/Tesaro, Merck, and Verastem; Associate Director for GOG Partners; NRG ovarian chair; and on the GOG Foundation BOD. AO: consultancy fees from AstraZeneca, MSD/Merck, Clovis Oncology, Genmab, Immunogen, PharmaMar, Roche, Tesaro, GSK, Deciphera, Novocure, SUTRO, Akesobio, Mersana Therapeutics, and Shattucklabs; institutional financial interests (research funding) from AbbVie Deutschland, Ability Pharmaceuticals, Advaxis, Aeterna Zentaris, Amgen, SA, Aprea Therapeutics AB, Clovis Oncology, Eisai, F. Hoffmann-La Roche, and Regeneron Pharmaceuticals; travel, accommodations and expenses fees from AstraZeneca, Clovis Oncology, PharmaMar, and Roche. SD: consulting fees for AstraZeneca Pharma, Novartis Pharmaceu, Pfizer Genentech USA, Puma Biotechnology, Amgen, Lilly, AbbVie, Lexicon Pharmaceutical, Eisai, Seagen, Daiichi Sankyo, and Clovis Oncology. LJC: personal fees from Celsion Corporation, Elevar Therapeutics, Myriad Genetics, Rubius Therapeutics, Sorrento Therapeutics, Tarveda Therapeutics, Toray Industries, VBL Therapeutics, OncoNova, Inx Med, and Luzsana Biotechnology; personal fees and other from Corcept Therapeutics; grants and personal fees from GSK and Immunogen; grants from Abbvie, Advaxis, Agenus, Ajinomoto, Array BioPharm, AstraZeneca, Bristol Myers Squibb, Clovis Oncology, Deciphera Parma, Eisai, EMD Serono, ERGOMED Clinical Research, Exelixis, Genentech/Roche, Genmab, Hoffman-LaRoche, Incyte Corporation, Iovance Biotherapeutics, InVentive Health Clinical, Jansen R&D, Leap Therapeutics, Ludwig Institute for Pharmaceuticals, Merck, Mersana Therapeutics, Novocure, Novartis Pharmaceuticals, OncoQuest, PRA International, Regeneron Pharmaceuticals, Seattle Genetics, Serono, Sutro Biopharm, Tesaro (GSK), Arcus Biosciences, Sumitomo Dainippon Pharma Oncolgy, Cerulean Pharma, Karyopharm, BeiGene USA, Ovagene, Pfizer, Pharma Mar USA, Precision Therapeutics, Sanofi, Stemcentrx, TRACON Pharm, and Verastem. BJM: consultant for Acrivon, Adaptimune, Agenus, Akeso Bio, Amgen, Aravive, Bayer, Elevar, EMD Merck, Genmab/Seagen, GOG Foundation, Heng Rui, ImmunoGen, Karyopharm, Iovance, Laekna, Macrogenics, Mersana, Novartis, Novocure, OncoC4, Panavance, Pieris, Pfizer, Puma, Regeneron, Sorrento, VBL, Verastem, and Zentalis; speaker/consultant for AstraZeneca, Clovis, Eisai, Merck, Myriad, Roche/Genentech, and TESARO/GSK; consultant and investigator for Gradalis and US Oncology Research. RLC: grants from Merck, personal fees from GSK, Agenus, Regeneron, and OncoQuest; grants and personal fees from Clovis, Genmab, Roche/Genentech, Janssen, and AstraZeneca. TH: Scientific Advisory Board for AstraZeneca, Aravive, Caris, Clovis, Eisai, Epsilogen, Genentech/Roche, Gradalis, GSK, and Merck. JS and AS: employment and shares: Bayer AG. LK, ASchulz, KK, AW, BC, and CE: employment: Bayer AG.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
