

Ross Procedure Versus Mechanical Versus Bioprosthetic Aortic Valve Replacement: A Network Meta-Analysis
- PMID: 36565200
- PMCID: PMC9973571
- DOI: 10.1161/JAHA.122.027715
Ross Procedure Versus Mechanical Versus Bioprosthetic Aortic Valve Replacement: A Network Meta-Analysis
Abstract
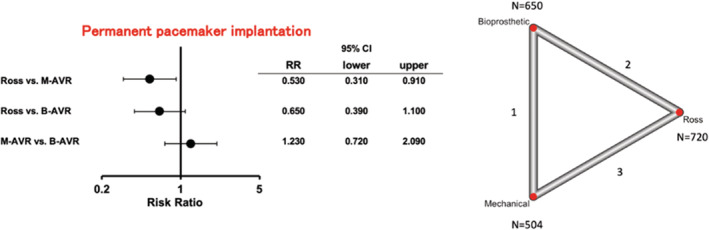
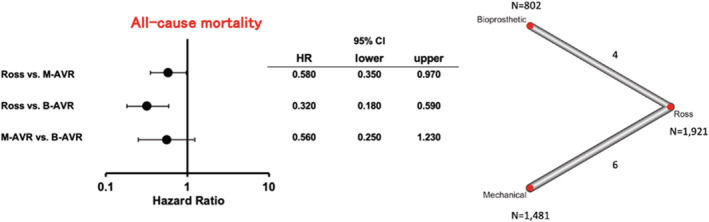
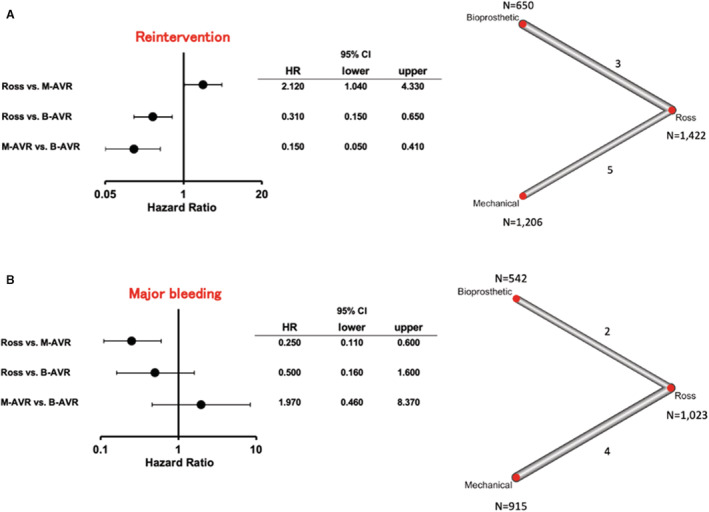
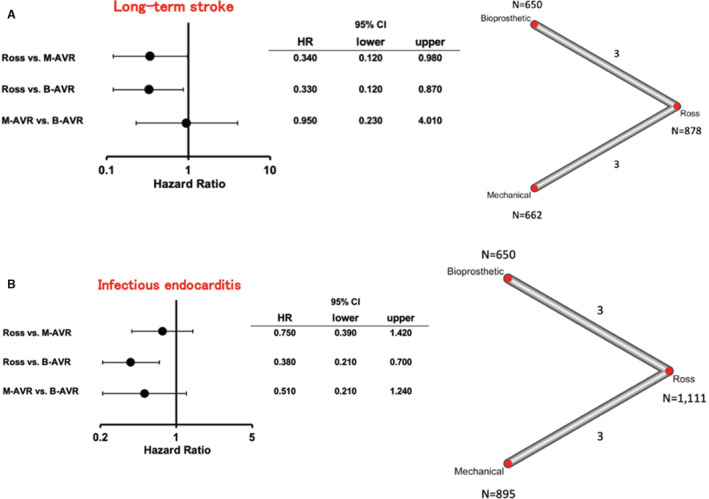
Background The Ross operation appears to restore normal survival in young and middle-aged adults with aortic valve disease. However, there are limited data comparing it with conventional aortic valve replacement. Herein, we compared outcomes of the Ross procedure with mechanical and bioprosthetic aortic valve replacement (M-AVR and B-AVR, respectively). Methods and Results MEDLINE and EMBASE were searched through March 2022 to identify randomized controlled trials and propensity score-matched studies that investigated outcomes of patients aged ≥16 years undergoing the Ross procedure, M-AVR, or B-AVR. The systematic literature search identified 2 randomized controlled trials and 8 propensity score-matched studies involving a total of 4812 patients (Ross: n=1991; M-AVR: n=2019; and B-AVR: n=802). All-cause mortality was significantly lower in the Ross procedure group compared with M-AVR (hazard ratio [HR] [95% CI], 0.58 [0.35-0.97]; P=0.035) and B-AVR (HR [95% CI], 0.32 [0.18-0.59]; P<0.001) groups. The reintervention rate was lower after the Ross procedure and M-AVR compared with B-AVR, whereas it was higher after the Ross procedure compared with M-AVR. Major bleeding rate was lower after the Ross procedure compared with M-AVR. Long-term stroke rate was lower following the Ross procedure compared with M-AVR and B-AVR. The rate of endocarditis was also lower after the Ross procedure compared with B-AVR. Conclusions Improved long-term outcomes of the Ross procedure are demonstrated compared with conventional M-AVR and B-AVR options. These results highlight a need to enhance the recognition of the Ross procedure and revisit current guidelines on the optimal valve substitute for young and middle-aged patients.
Keywords: Ross procedure; aortic valve substitute; bioprosthetic aortic valve replacement; mechanical aortic valve replacement; surgical aortic valve replacement.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
