

Novel PGM3 mutation in two siblings with combined immunodeficiency and childhood bullous pemphigoid: a case report and review of the literature
- PMID: 36566211
- PMCID: PMC9789581
- DOI: 10.1186/s13223-022-00749-0
Novel PGM3 mutation in two siblings with combined immunodeficiency and childhood bullous pemphigoid: a case report and review of the literature
Abstract
Background: Bullous pemphigoid is the most common autoimmune subepidermal blistering disorder with a low incidence in childhood. Combined immunodeficiencies (CIDs) are a group of monogenic inborn errors of immunity (IEIs) characterized by T- and B-cell dysfunction leading to recurrent infections, lymphoproliferation, predisposition to malignancy, and autoimmunity. Here, we report two Afghan siblings with a diagnosis of CID and extremely rare manifestation of diffuse bullous pemphigoid skin lesions.
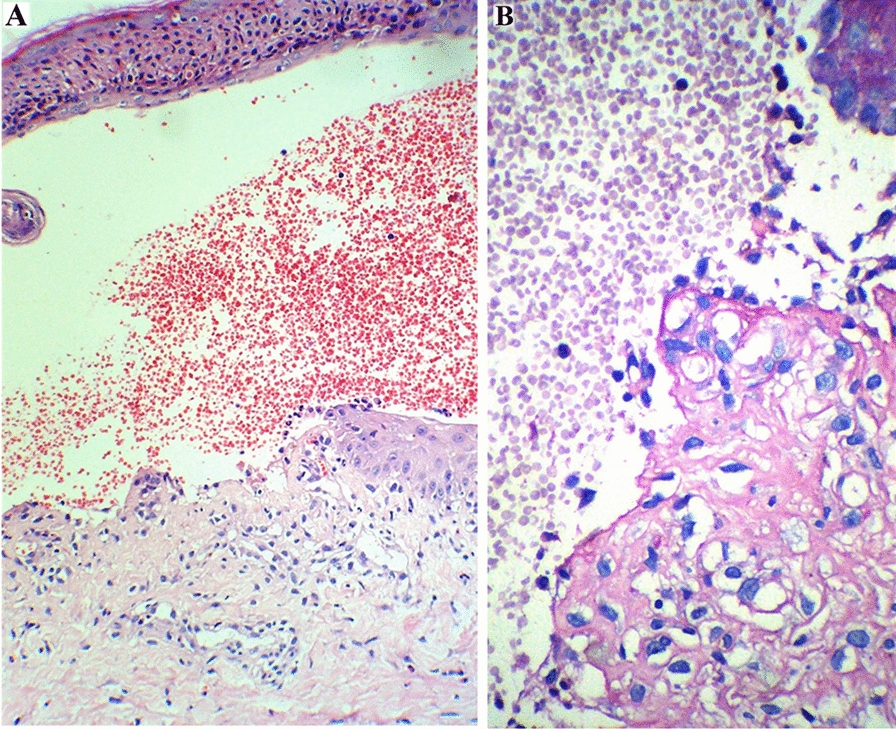
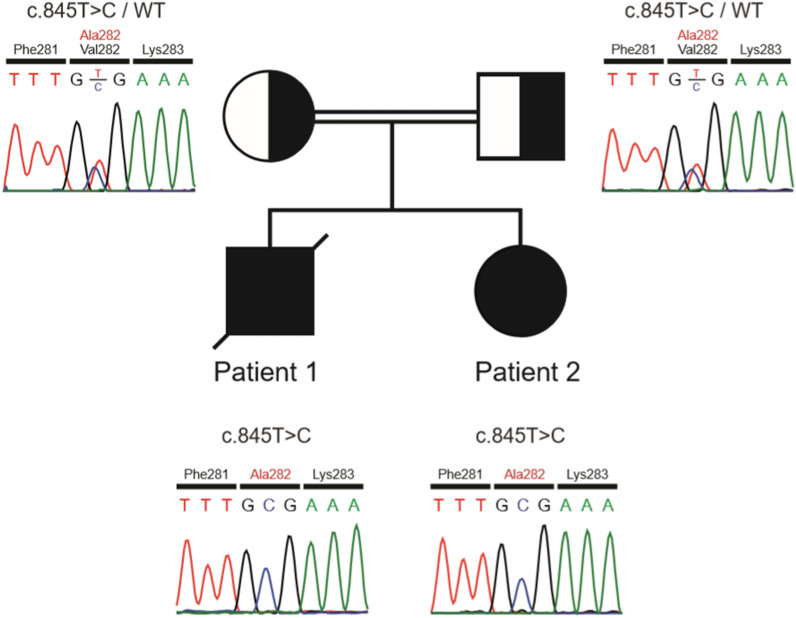
Case presentation: The older sibling (patient 1) was a 32-month-old male with facial dysmorphism, protracted diarrhea, failure to thrive, recurrent oral candidiasis, recurrent otitis media with tympanic membrane perforation, who had been previously diagnosed with CID. While he was under treatment with intravenous immunoglobulin (IVIg), he developed extensive blistering lesions, which were diagnosed as childhood bullous pemphigoid. Methylprednisolone and azathioprine were added to the regimen, which resulted in a remarkable improvement of the skin lesions and also the feeding condition. However,2 weeks later, he was re-admitted to the intensive care unit (ICU) and eventually died due to fulminant sepsis. Later, his 12-month-old sister (patient 2) with similar facial dysmorphism and a history of developmental delay, food allergy, recurrent oral candidiasis, and respiratory tract infections also developed blistering skin lesions. She was under treatment for occasional eczematous lesions, and had been receiving IVIg for 3 months due to low levels of immunoglobulins. Further immunologic workup showed an underlying CID and thus treatment with IVIg continued, gradually improving her clinical condition. The genetic study of both siblings revealed a novel homozygous mutation in exon 7 of the PGM3 gene, c.845 T > C (p.Val282Ala).
Conclusions: Dermatologic disorders may be the presenting sign in patients with CID and mutated PGM3. This case report further extends the spectrum of skin manifestations that could be observed in PGM3 deficiency and emphasizes the importance of considering CIDs during the assessment of skin disorders, particularly if they are extensive, recurrent, refractory to treatment, and/or associated with other signs of IEIs.
Keywords: Blister; Case report; Inborn errors of immunity; PGM3 deficiency; Skin.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Chou C-S. Childhood bullous pemphigoid: a case report and literature review. J Clin Exp Dermatol Res. 2014 doi: 10.4172/2155-9554.S6-010. - DOI
-
- Tangye SG, Al-Herz W, Bousfiha A, Chatila T, Cunningham-Rundles C, Etzioni A, et al. Human inborn errors of immunity: 2019 update on the classification from the international union of immunological societies expert committee. J Clin Immunol. 2020;40(1):24–64. doi: 10.1007/s10875-019-00737-x. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
