

Understanding clinical and biological heterogeneity to advance precision medicine in paediatric acute respiratory distress syndrome
- PMID: 36566767
- PMCID: PMC10880453
- DOI: 10.1016/S2213-2600(22)00483-0
Understanding clinical and biological heterogeneity to advance precision medicine in paediatric acute respiratory distress syndrome
Abstract
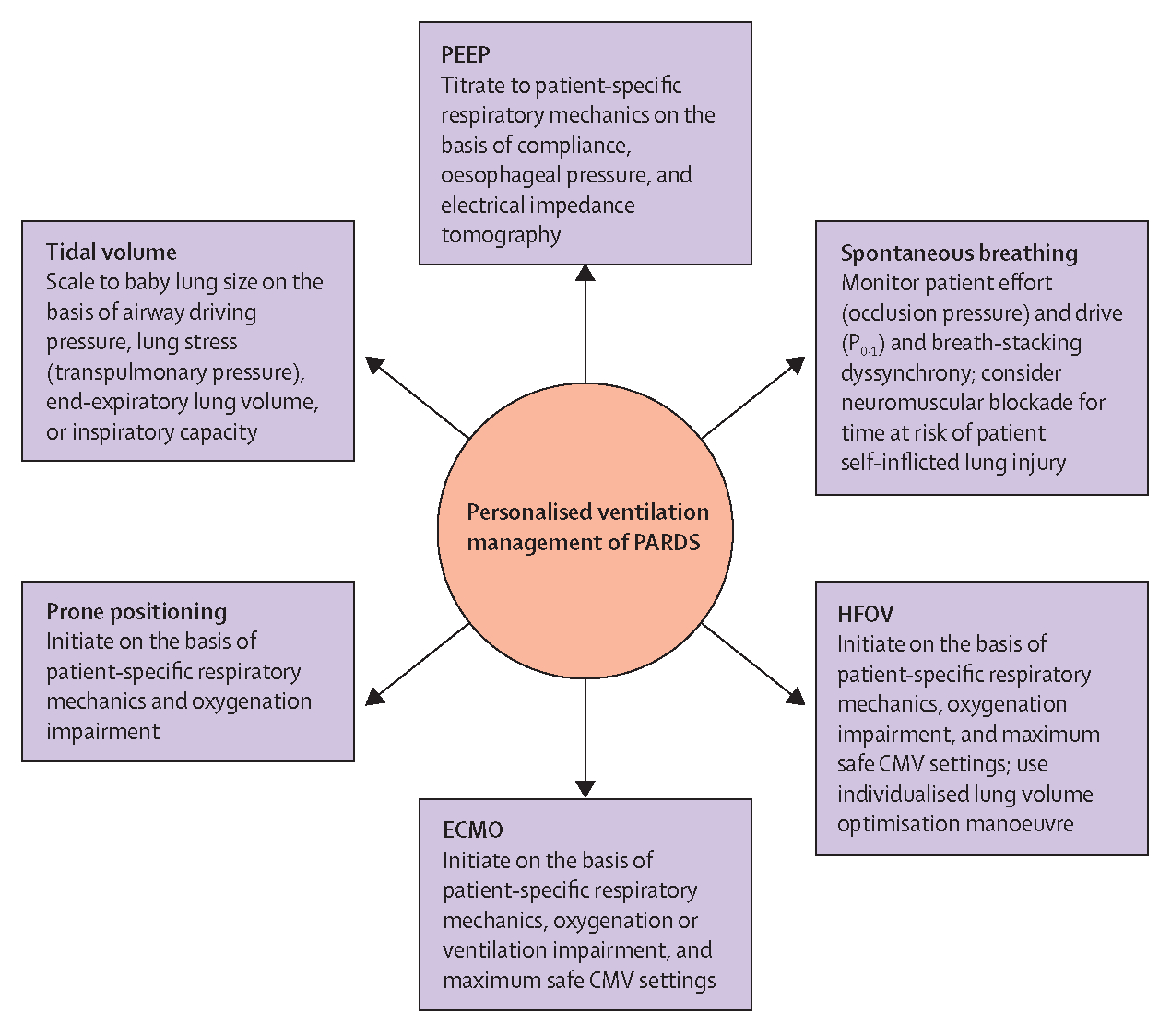
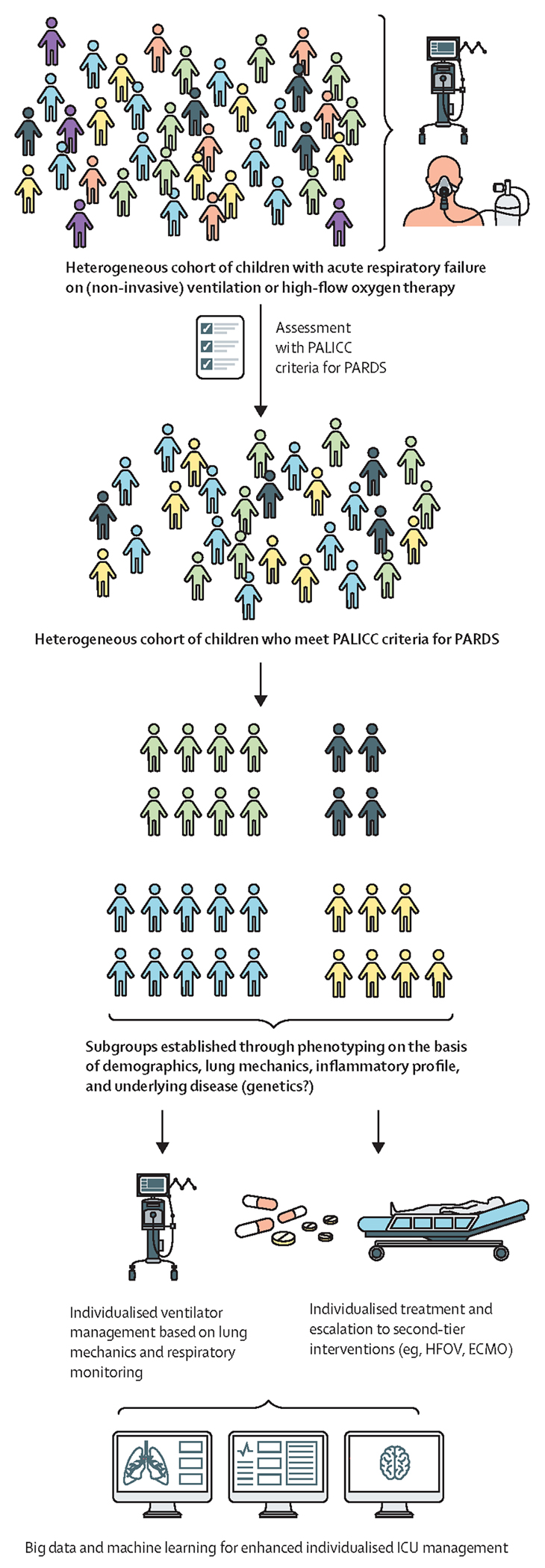
Paediatric acute respiratory distress syndrome (PARDS) is a heterogeneous clinical syndrome that is associated with high rates of mortality and long-term morbidity. Factors that distinguish PARDS from adult acute respiratory distress syndrome (ARDS) include changes in developmental stage and lung maturation with age, precipitating factors, and comorbidities. No specific treatment is available for PARDS and management is largely supportive, but methods to identify patients who would benefit from specific ventilation strategies or ancillary treatments, such as prone positioning, are needed. Understanding of the clinical and biological heterogeneity of PARDS, and of differences in clinical features and clinical course, pathobiology, response to treatment, and outcomes between PARDS and adult ARDS, will be key to the development of novel preventive and therapeutic strategies and a precision medicine approach to care. Studies in which clinical, biomarker, and transcriptomic data, as well as informatics, are used to unpack the biological and phenotypic heterogeneity of PARDS, and implementation of methods to better identify patients with PARDS, including methods to rapidly identify subphenotypes and endotypes at the point of care, will drive progress on the path to precision medicine.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests MCJK reports personal fees from Vyaire and Metran, and research funding from Vyaire and Applied Biosignals, outside of the submitted work. RGK reports personal fees from Orange Med Nihon Kohden; he has received reimbursement for participation on data safety monitoring boards for the PREVENT study (funded by the NIH) and the FIRST-ABC study (funded by the UK National Institute for Health and Care Research), outside of the submitted work. GE has received financial support from Maquet for an investigator-led study, outside of the submitted work. PCR has received personal fees from Getinge, outside of the submitted work. The other authors declare no competing interests.
Figures
Comment in
-
Addressing the inequity of acute respiratory distress syndrome.Lancet Respir Med. 2023 Feb;11(2):119-121. doi: 10.1016/S2213-2600(22)00352-6. Epub 2022 Sep 4. Lancet Respir Med. 2023. PMID: 36070794 No abstract available.
-
The future of paediatric acute respiratory distress syndrome.Lancet Respir Med. 2023 Feb;11(2):121-123. doi: 10.1016/S2213-2600(22)00358-7. Epub 2022 Dec 22. Lancet Respir Med. 2023. PMID: 36566766 Free PMC article. No abstract available.
References
-
- Schouten LR, Veltkamp F, Bos AP, et al. Incidence and mortality of acute respiratory distress syndrome in children: a systematic review and meta-analysis. Crit Care Med 2016; 44: 819–29. - PubMed
-
- Quasney MW, Lopez-Fernandez YM, Santschi M, Watson RS, Pediatric Acute Lung Injury Consensus Conference Group. The outcomes of children with pediatric acute respiratory distress syndrome: proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med 2015; 16: S118–31. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet 1967; 2: 319–23. - PubMed
-
- Thomas NJ, Jouvet P, Willson D. Acute lung injury in children--kids really aren’t just “little adults”. Pediatr Crit Care Med 2013; 14: 429–32. - PubMed
-
- Flori HR, Glidden DV, Rutherford GW, Matthay MA. Pediatric acute lung injury: prospective evaluation of risk factors associated with mortality. Am J Respir Crit Care Med 2005; 171: 995–1001. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
