

Incidence, costs and post-operative complications following ankle fracture - A US claims database analysis
- PMID: 36567314
- PMCID: PMC9791722
- DOI: 10.1186/s12891-022-06095-x
Incidence, costs and post-operative complications following ankle fracture - A US claims database analysis
Abstract
Background: The epidemiology and payer costs for ankle fractures are not well documented. This study evaluated: (1) the incidence of ankle fracture and ankle surgery following fracture in the US population; and (2) the clinical presentation of patients presenting with ankle fractures requiring surgery, their complication rates, and payer costs.
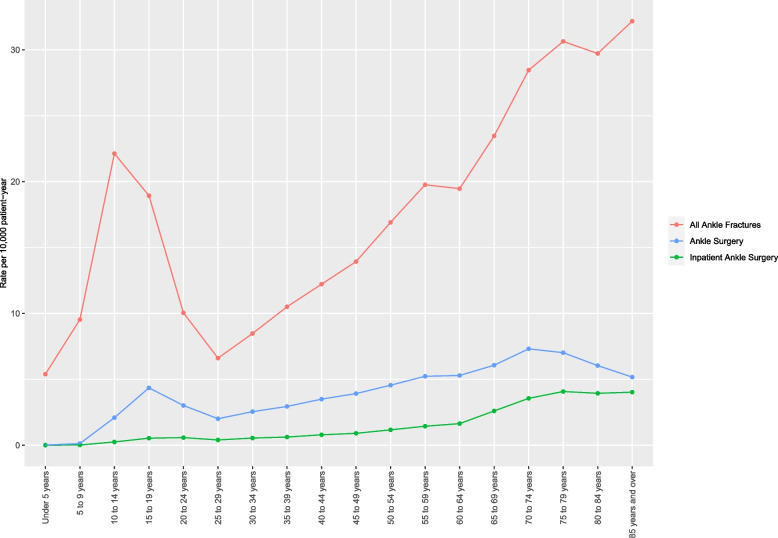
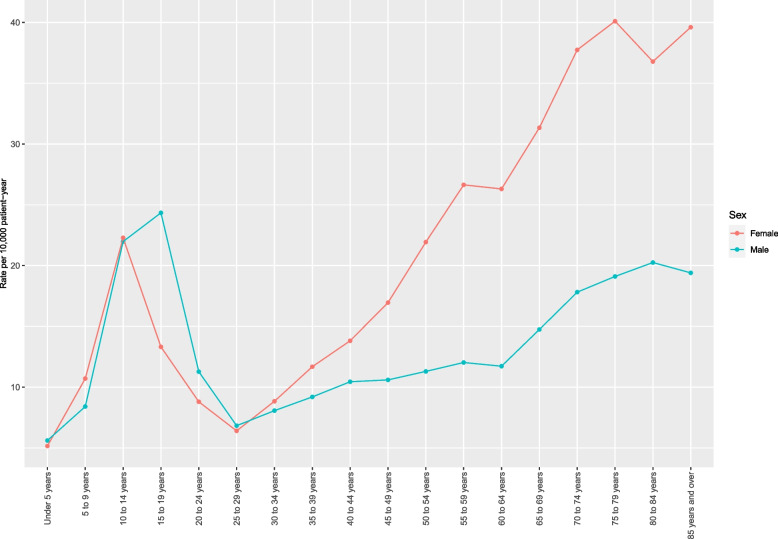
Methods: Patients in the IBM® MarketScan® Commercial and Medicare Supplemental databases with an inpatient/outpatient diagnosis of ankle fracture from 2016 to 2019 were stratified by age group and gender, and rates of fracture per 10,000 enrollees were estimated. Surgically-treated patients between January 2016 - October 2021 were further analyzed. One-year post-surgical outcomes evaluated complication rates (e.g., infection, residual pain), reoperations, and 1-year payments. Standard descriptive statistics were calculated for all variables and outcomes. Generalized linear models were designed to estimate payments for surgical care and incremental payments associated with postoperative complications.
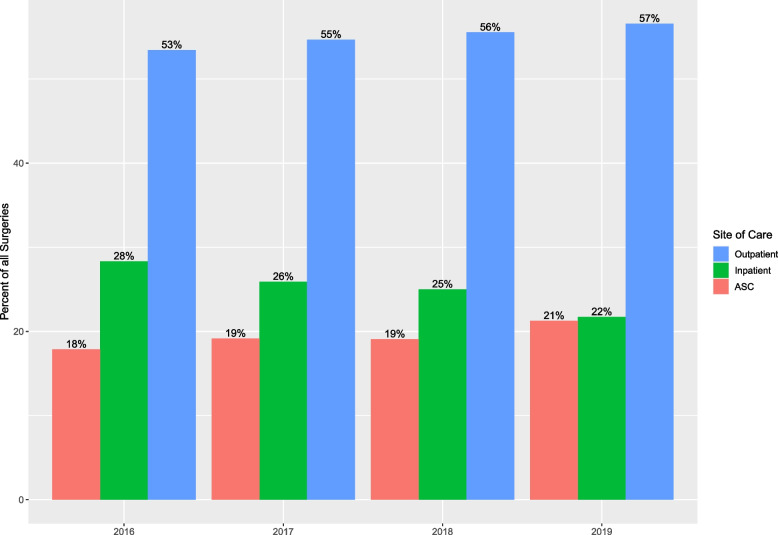
Results: Fracture cases affected 0.14% of the population; 23.4% of fractures required surgery. Pediatric and elderly patients were at increased risk. From 3 weeks to 12 months following index ankle surgery, 5.5% (5.3% - 5.7%) of commercially insured and 5.9% (5.1% - 6.8%) of Medicare patients required a new surgery. Infection was observed in 4.4% (4.2% - 4.6%) commercially insured and 9.8% (8.8% - 10.9%) Medicare patients, and residual pain 3 months post-surgery was observed in 29.5% (28.7% - 30.3%) commercially-insured and 39.3% (36.0% - 42.6%) Medicare patients. Commercial payments for index surgery ranged from $9,821 (95% CI: $9,697 - $9,945) in the ambulatory surgical center to $28,169 (95% CI: $27,780 - $28,559) in the hospital inpatient setting, and from $16,775 (95% CI: $16,668 - $16,882) in patients with closed fractures, to $41,206 (95% CI: $38,795 - $43,617) in patients with Gustilo III fractures. Incremental commercial payments for pain and infection averaged $5,200 (95% CI: $4,261 - $6,139) and $27,510 (95% CI: $21,759 - $33,261), respectively.
Conclusion: Ankle fracture has a high incidence and complication rate. Residual pain affects more than one-third of all patients. Ankle fracture thus presents a significant societal impact in terms of patient outcomes and payer burden.
Keywords: Ankle fractures; Claims database; Comorbidities; Complications; Costs; Infection; Pain; Payments; Reoperation.
© 2022. The Author(s).
Conflict of interest statement
All authors are employees of Johnson & Johnson (JnJ) or DePuy Synthes (a JnJ Company) and receive salary and/or own stock in JnJ.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
