

Mechanical ventilation in patients with cardiogenic pulmonary edema: a sub-analysis of the LUNG SAFE study
- PMID: 36567347
- PMCID: PMC9791731
- DOI: 10.1186/s40560-022-00648-x
Mechanical ventilation in patients with cardiogenic pulmonary edema: a sub-analysis of the LUNG SAFE study
Abstract
Background: Patients with acute respiratory failure caused by cardiogenic pulmonary edema (CPE) may require mechanical ventilation that can cause further lung damage. Our aim was to determine the impact of ventilatory settings on CPE mortality.
Methods: Patients from the LUNG SAFE cohort, a multicenter prospective cohort study of patients undergoing mechanical ventilation, were studied. Relationships between ventilatory parameters and outcomes (ICU discharge/hospital mortality) were assessed using latent mixture analysis and a marginal structural model.
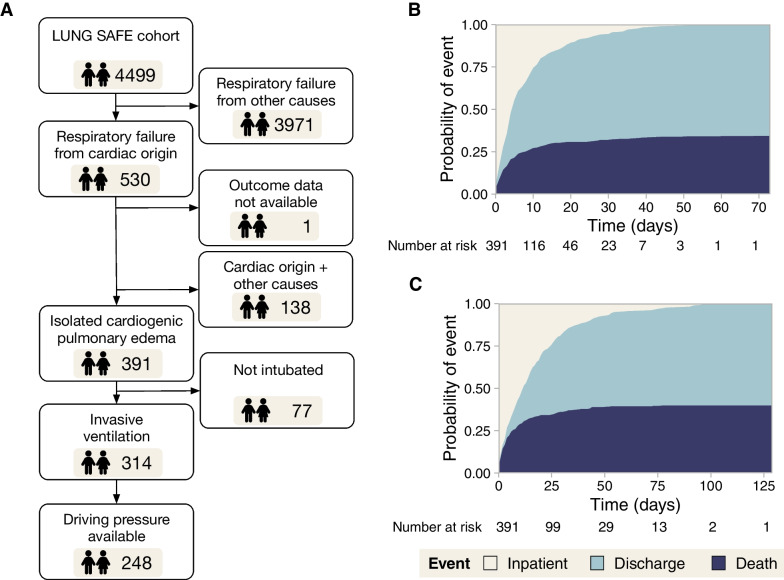
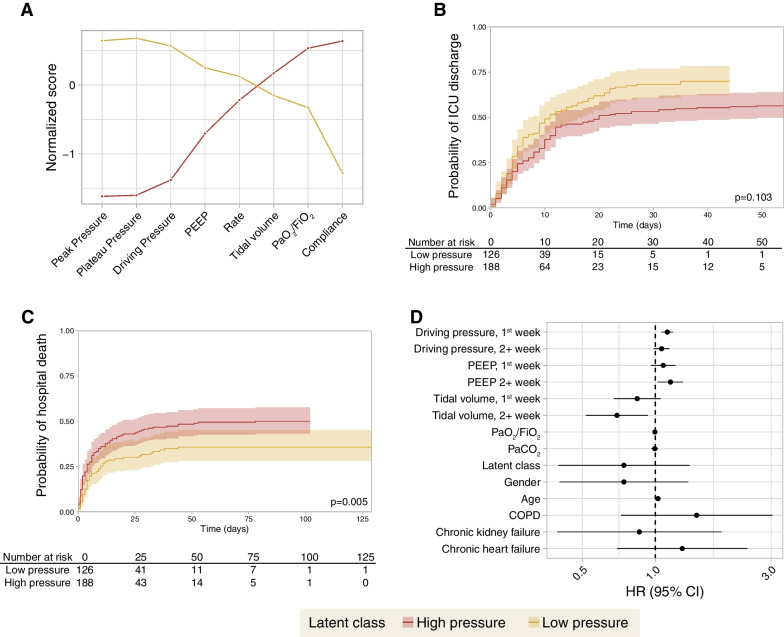
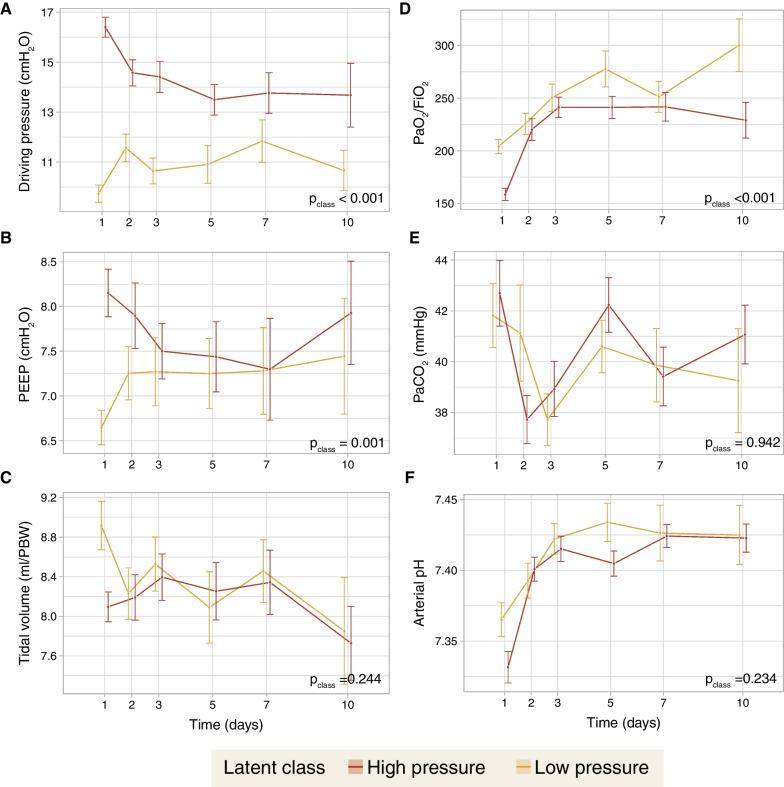
Results: From 4499 patients, 391 meeting CPE criteria (median age 70 [interquartile range 59-78], 40% female) were included. ICU and hospital mortality were 34% and 40%, respectively. ICU survivors were younger (67 [57-77] vs 74 [64-80] years, p < 0.001) and had lower driving (12 [8-16] vs 15 [11-17] cmH2O, p < 0.001), plateau (20 [15-23] vs 22 [19-26] cmH2O, p < 0.001) and peak (21 [17-27] vs 26 [20-32] cmH2O, p < 0.001) pressures. Latent mixture analysis of patients receiving invasive mechanical ventilation on ICU day 1 revealed a subgroup ventilated with high pressures with lower probability of being discharged alive from the ICU (hazard ratio [HR] 0.79 [95% confidence interval 0.60-1.05], p = 0.103) and increased hospital mortality (HR 1.65 [1.16-2.36], p = 0.005). In a marginal structural model, driving pressures in the first week (HR 1.12 [1.06-1.18], p < 0.001) and tidal volume after day 7 (HR 0.69 [0.52-0.93], p = 0.015) were related to survival.
Conclusions: Higher airway pressures in invasively ventilated patients with CPE are related to mortality. These patients may be exposed to an increased risk of ventilator-induced lung injury. Trial registration Clinicaltrials.gov NCT02010073.
Keywords: Cardiogenic pulmonary edema; Driving pressure; Mechanical ventilation; Ventilator-induced lung injury.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests to disclose.
Figures
References
-
- Vergani G, Cressoni M, Crimella F, L’Acqua C, Sisillo E, Gurgitano M, et al. A morphological and quantitative analysis of lung CT scan in patients with acute respiratory distress syndrome and in cardiogenic pulmonary edema. J Intensive Care Med. 2020;35:284–292. doi: 10.1177/0885066617743477. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
