

Physiologic Effects of the Awake Prone Position Combined With High-Flow Nasal Oxygen on Gas Exchange and Work of Breathing in Patients With Severe COVID-19 Pneumonia: A Randomized Crossover Trial
- PMID: 36567785
- PMCID: PMC9760623
- DOI: 10.1097/CCE.0000000000000805
Physiologic Effects of the Awake Prone Position Combined With High-Flow Nasal Oxygen on Gas Exchange and Work of Breathing in Patients With Severe COVID-19 Pneumonia: A Randomized Crossover Trial
Abstract
To determine the effect of the awake prone position (APP) on gas exchange and the work of breathing in spontaneously breathing patients with COVID-19-associated acute hypoxemic respiratory failure (AHRF) supported by high-flow nasal oxygen.
Design: Prospective randomized physiologic crossover multicenter trial.
Settings: Four ICUs in Marseille, France.
Patients: Seventeen patients with laboratory-confirmed COVID-19 pneumonia and Pao2/Fio2 less than or equal to 300 mm Hg while treated with high-flow nasal cannula oxygen therapy.
Interventions: Periods of APP and semirecumbent position (SRP) were randomly applied for 2 hours and separated by a 2-hour washout period.
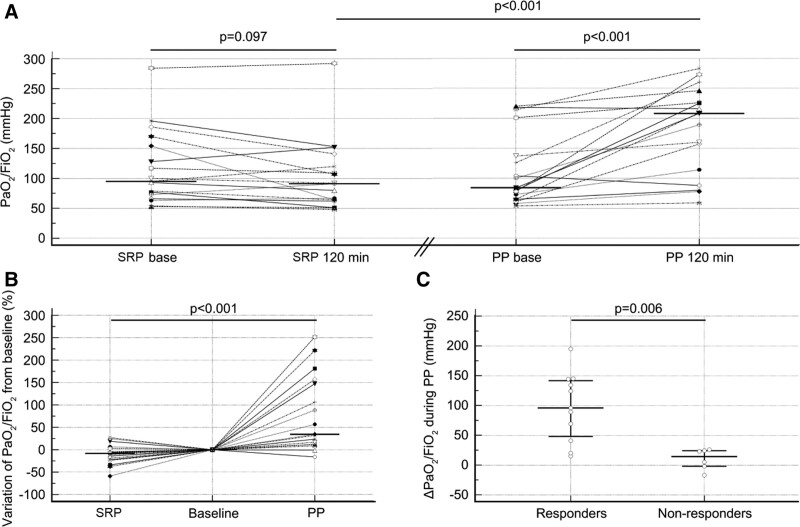
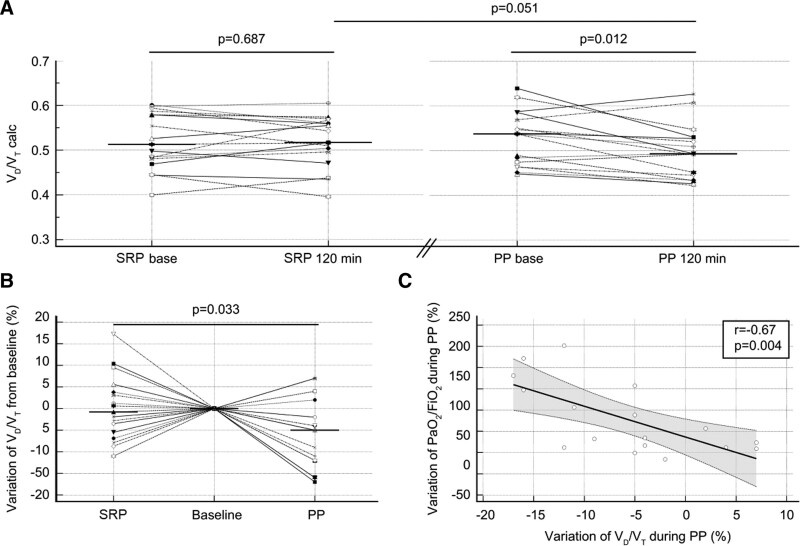
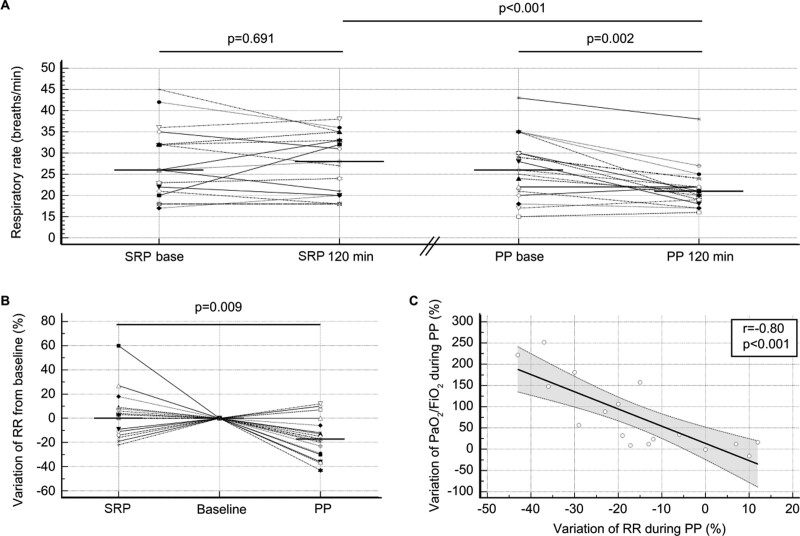
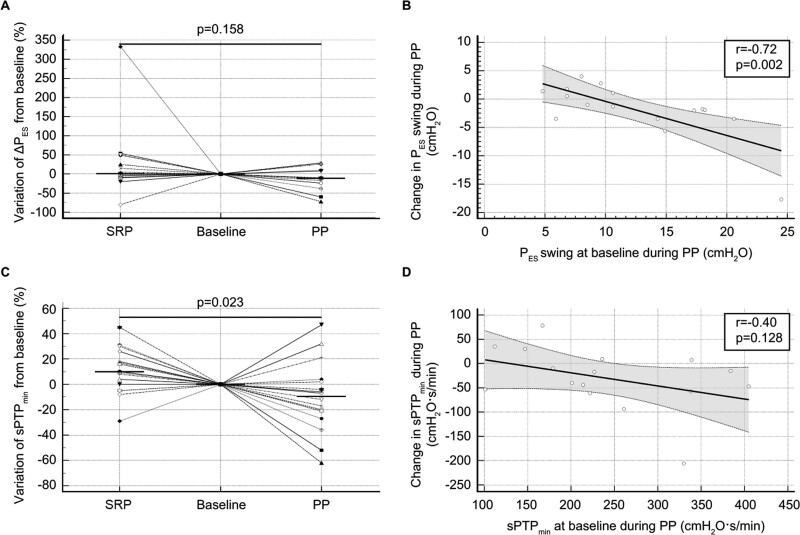
Measurements and main results: Arterial blood gases, end-tidal CO2. and esophageal pressure were recorded prior to and at the end of each period. Inspiratory muscle effort was assessed by measuring the esophageal pressure swing (∆PES) and the simplified esophageal pressure-time product (sPTPES). The other endpoints included physiologic dead space to tidal volume ratio (VD/VT) and the transpulmonary pressure swing. The APP increased the Pao2/Fio2 from 84 Torr (61-137 Torr) to 208 Torr (114-226 Torr) (p = 0.0007) and decreased both the VD/VT and the respiratory rate from 0.54 (0.47-0.57) to 0.49 (0.45-0.53) (p = 0.012) and from 26 breaths/min (21-30 breaths/min) to 21 breaths/min (19-22 breaths/min), respectively (p = 0.002). These variables remained unchanged during the SRP. The ∆PES and sPTPES per breath were unaffected by the position. However, the APP reduced the sPTPES per minute from 225 cm H2O.s.m-1 (176-332 cm H2O.s.m-1) to 174 cm H2O.s.m-1 (161-254 cm H2O.s.m-1) (p = 0.049).
Conclusions: In spontaneously breathing patients with COVID-19-associated AHRF supported by high-flow nasal oxygen, the APP improves oxygenation and reduces the physiologic dead space, respiratory rate, and work of breathing per minute.
Keywords: COVID-19; prone position; respiratory distress syndrome; respiratory insufficiency; work of breathing.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Ospina-Tascón GA, Calderón-Tapia LE, García AF, et al. ; HiFLo-Covid Investigators: Effect of high-flow oxygen therapy vs conventional oxygen therapy on invasive mechanical ventilation and clinical recovery in patients with severe COVID-19: A randomized clinical trial. JAMA 2021; 326:2161–2171 - PMC - PubMed
LinkOut - more resources
Full Text Sources
