

Intraoperative assessment of bone viability through improved analysis and visualization of dynamic contrast-enhanced fluorescence imaging: technique report
- PMID: 36569105
- PMCID: PMC9782343
- DOI: 10.1097/OI9.0000000000000222
Intraoperative assessment of bone viability through improved analysis and visualization of dynamic contrast-enhanced fluorescence imaging: technique report
Abstract
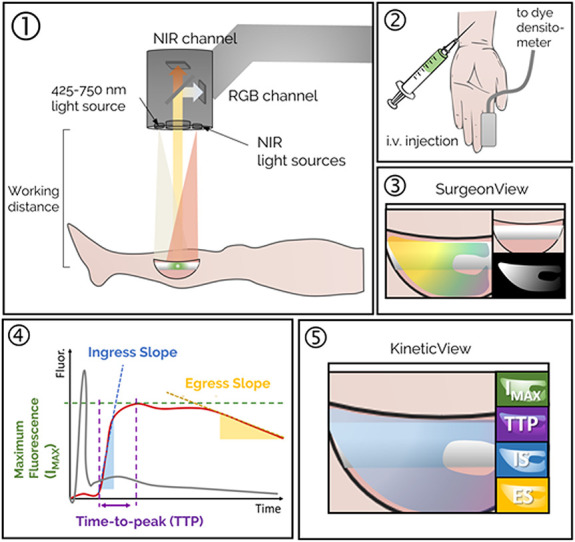
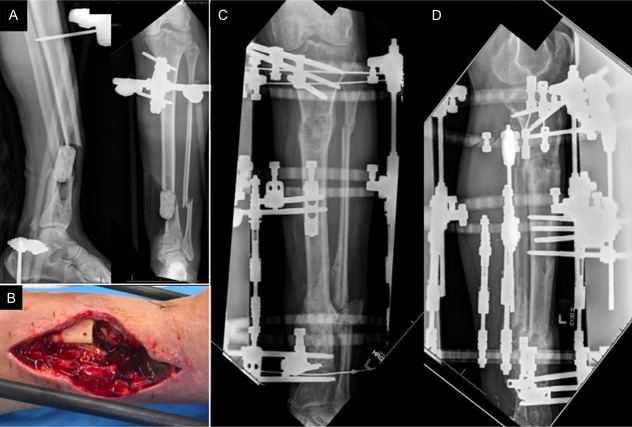
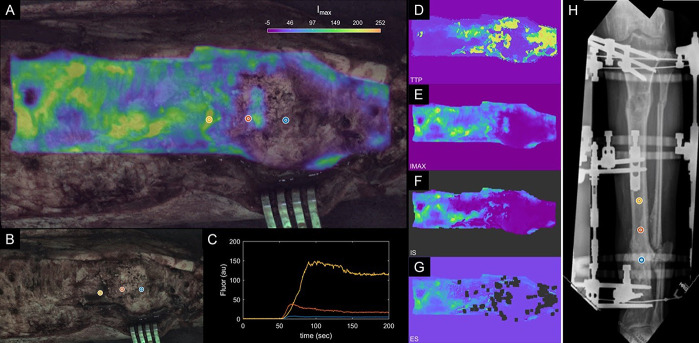
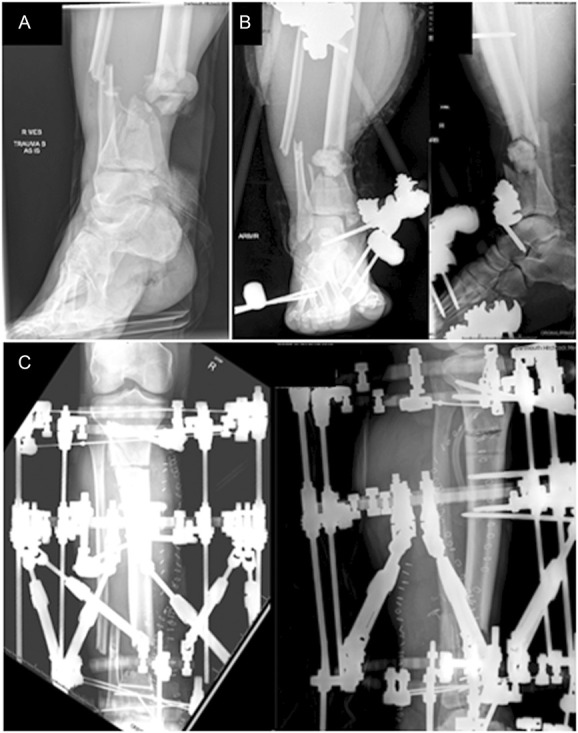
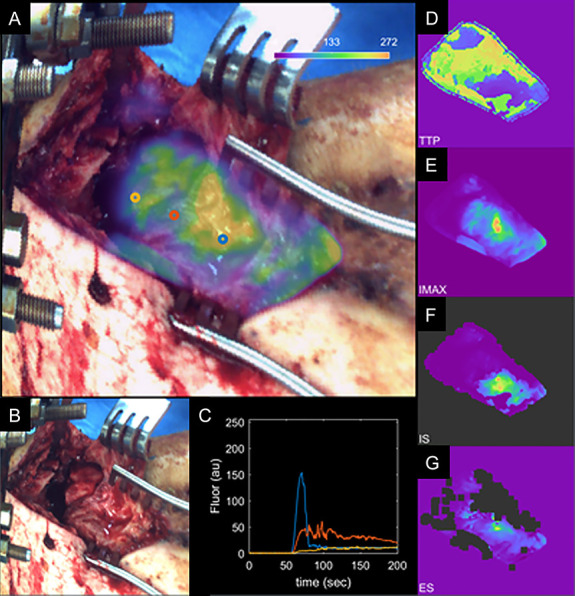
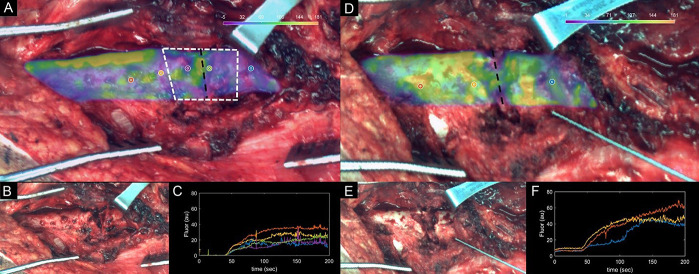
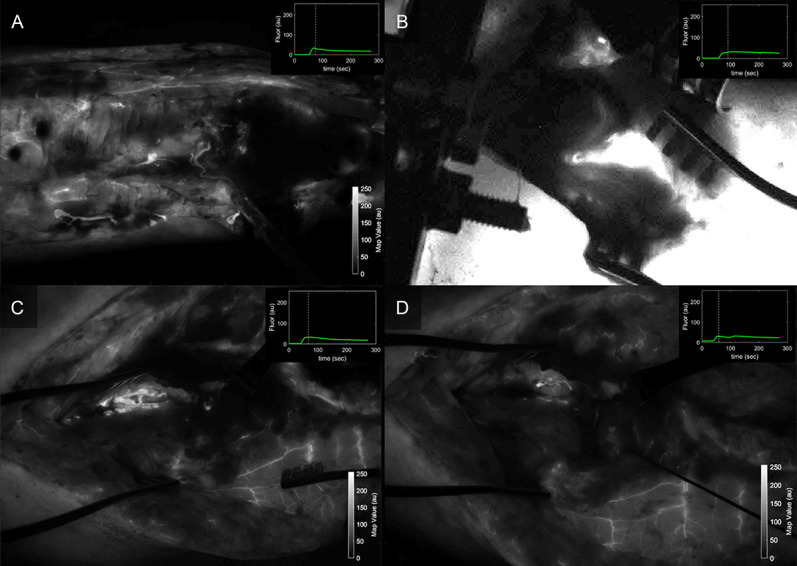
Bone devitalization is believed to be a critical determinant of complications such as infection or nonunion. However, intraoperative assessment of bone devitalization, particularly in open fractures and infections, remains highly subjective resulting in variation in treatment. Optical imaging tools, particularly dynamic contrast-enhanced fluorescence imaging, can provide real-time, intraoperative assessment of bone and soft tissue perfusion, which informs the tissues' ability to heal and fight infection. We describe a novel technique to apply indocyanine green-based fluorescence imaging, using a device that is frequently used in the operating room to assess skin or flap perfusion in plastic surgery, to assess bone and deep tissue perfusion in three pertinent cases: (1) a chronic infection/nonunion after a Gustilo type 3A tibia fracture (patient 1), (2) an acute Gustilo type 3C tibia open fracture with extensive degloving/soft tissue stripping (patient 2), and (3) an atrophic nonunion of the humerus (patient 3). In all three cases, fluorescence imaging (both time-specific fluorescence and maximum fluorescence) and derived kinetic maps of time-to-peak, ingress slope, and egress slope demonstrated clear spatial variation in perfusion that corresponded to the patient pathogenesis. The impact of this information on patient outcome will need to be evaluated in future clinical trials; however, these cases demonstrate in principle that optical imaging information has the potential to inform surgical practice, reduce the variation in treatment, and improve outcomes observed in these challenging patients.
Keywords: debridement; fluorescence-guided surgery; fracture fixation; open fracture; surgical wound infection; trauma.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Orthopaedic Trauma Association.
Conflict of interest statement
The authors report no conflict of interest.
Figures

References
-
- Yun HC, Murray CK, Nelson KJ, et al. Infection after orthopaedic trauma: prevention and treatment. J Orthop Trauma. 2016;30:S21–S26. - PubMed
-
- Metsemakers W-J, Morgenstern M, McNally MA, et al. Fracture-related infection: a consensus on definition from an international expert group. Injury. 2018;49:505–510. - PubMed
-
- Lowenberg DW, Buntic RF, Buncke GM, et al. Long-term results and costs of muscle flap coverage with Ilizarov bone transport in lower limb salvage. J Orthop Trauma. 2013;27:576–581. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources