

Pro-Inflammatory Alterations of Circulating Monocytes in Latent Tuberculosis Infection
- PMID: 36570965
- PMCID: PMC9772871
- DOI: 10.1093/ofid/ofac629
Pro-Inflammatory Alterations of Circulating Monocytes in Latent Tuberculosis Infection
Abstract
Background: Latent tuberculosis infection (LTBI) has been associated with increased cardiovascular risk. We investigated the activation and pro-inflammatory profile of monocytes in individuals with LTBI and their association with coronary artery disease (CAD).
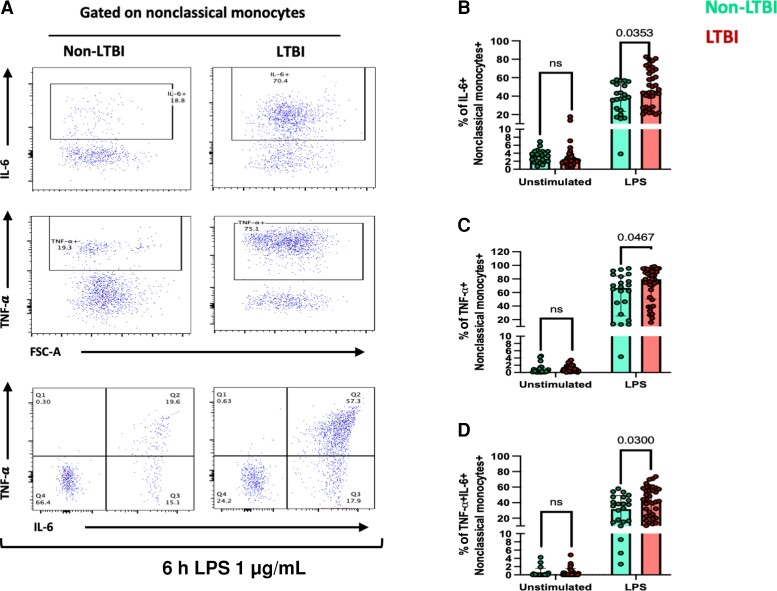
Methods: Individuals 40-70 years old in Lima, Peru, underwent QuantiFERON-TB testing to define LTBI, completed a coronary computed tomography angiography to evaluate CAD, and provided blood for monocyte profiling using flow cytometry. Cells were stimulated with lipopolysaccharide to assess interleukin-6 (IL-6) and tumor necrosis factor (TNF)-α responses.
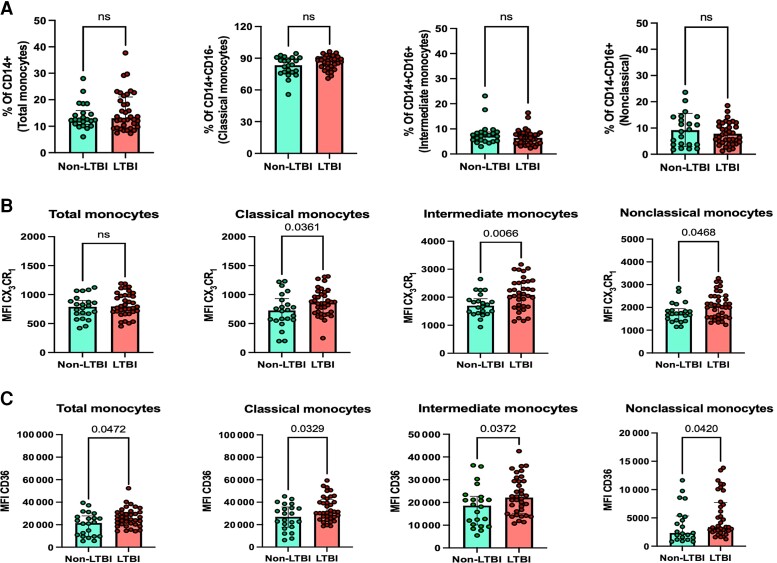
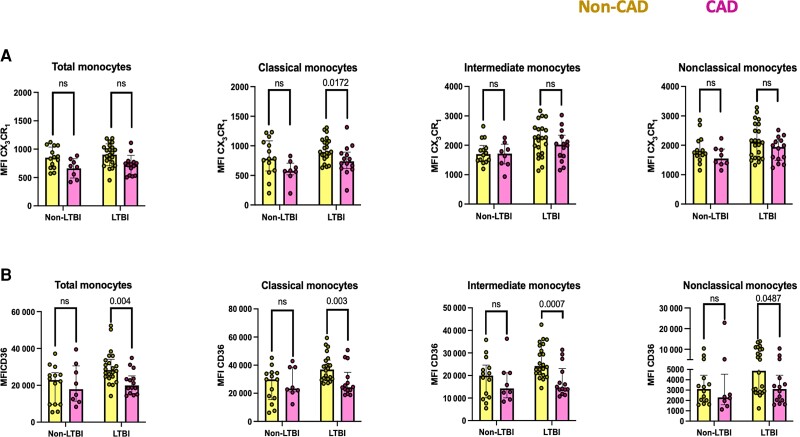
Results: The clinical characteristics of the LTBI (n = 28) and non-LTBI (n = 41) groups were similar. All monocyte subsets from LTBI individuals exhibited higher mean fluorescence intensity (MFI) of CX3CR1 and CD36 compared with non-LTBI individuals. LTBI individuals had an increased proportion of nonclassical monocytes expressing IL-6 (44.9 vs 26.9; P = .014), TNF-α (62.3 vs 35.1; P = .014), and TNF-α+IL-6+ (43.2 vs 36.6; P = .042). Among LTBI individuals, CAD was associated with lower CX3CR1 MFI on classical monocytes and lower CD36 MFI across all monocyte subsets. In multivariable analyses, lower CD36 MFI on total monocytes (b = -0.17; P = .002) and all subsets remained independently associated with CAD in LTBI.
Conclusions: Individuals with LTBI have distinct monocyte alterations suggestive of an exacerbated inflammatory response and tissue migration. Whether these alterations contribute to cardiovascular disease pathogenesis warrants further investigation.
Keywords: cardiovascular disease; coronary artery disease; inflammation; latent tuberculosis; monocytes.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. C. J. F. reports grants from Gilead Sciences, Inc., grants from ViiV Healthcare, Janssen, Amgen, Merck, and Cytodyn, and personal fees from Clinical Care Options, outside the submitted work. M.A.H. reports contracts from Gilead Sciences, Inc., and Insmed, Inc., to the University of Cincinnati, outside the submitted work. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Shah M, Dorman SE. Latent tuberculosis infection. N Engl J Med 2021; 385:2271–80. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
