

Can Molecular Classifications Help Tailor First-line Treatment of Metastatic Renal Cell Carcinoma? A Systematic Review of Available Models
- PMID: 36573246
- PMCID: PMC9789383
- DOI: 10.1016/j.euros.2022.11.006
Can Molecular Classifications Help Tailor First-line Treatment of Metastatic Renal Cell Carcinoma? A Systematic Review of Available Models
Abstract
Context: The advent of immune check inhibitors (ICIs) has tremendously changed the prognosis of metastatic renal cell carcinoma (mRCC), adding an unseen substantial overall survival benefit. These agents could be administered alone or in combination with anti-vascular endothelial growth factor (anti-VEGF) therapies. So far, treatment allocation is based only on clinical stratification risk models.
Objective: Herein, we aimed to report the different molecular classifications reported in the first-line treatment of mRCC and discuss the awaited clinical implications in terms of treatment selection.
Evidence acquisition: Medline database as well as European Society for Medical Oncology (ESMO)/American Society of Clinical Oncology (ASCO) conference proceedings were searched to identify biomarker studies. Inclusion criteria comprised randomized and nonrandomized clinical trials that included patients treated in the first line of mRCC setting, patients treated with anti-VEGF therapies or ICIs, biological modeling, and available survival outcomes.
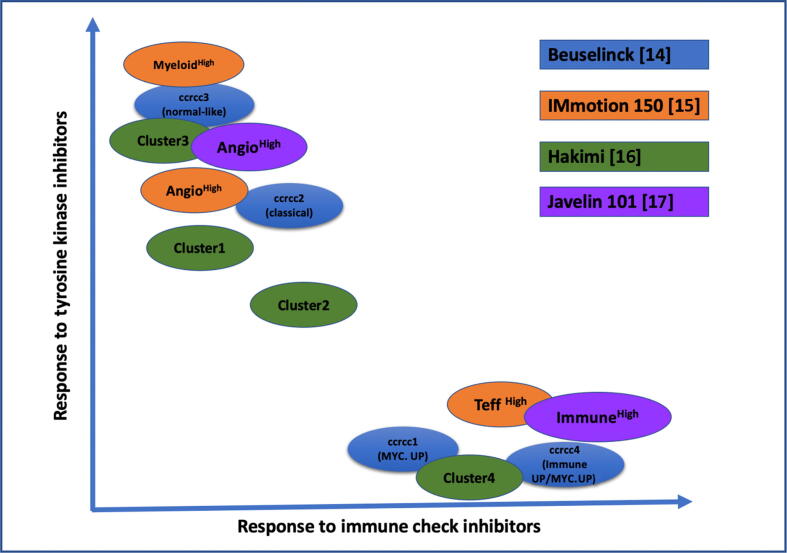
Evidence synthesis: Four classification models were identified with subsequent clinical implications: Beuselinck model (34 gene signatures), IMmotion150, Hakimi, and JAVELIN 101 model. Tumor profiling shows distinct outcomes when treated with one or other combination. Patients are clustered into two gene signatures: angiogenic and proinflammatory (as per JAVELIN). The first is more likely to respond to therapy that includes anti-VEGF agents, while the best outcomes are obtained with an ICI combination with the second.
Conclusions: The findings presented here were mostly derived from ancillary registered studies of new drugs in the setting of mRCC. Further validation is needed, which sets new paradigms for investigation in clinical research based on tumor biology for treatment allocation and not only on clinical stratification tools.
Patient summary: First-line treatment of metastatic kidney includes immunotherapy alone or in combination with antiangiogenic therapy. However, clinical practice demonstrated that the "one treatment fits all" strategy might not be the best approach. In fact, recent studies showed that the addition of immunotherapy agents will not benefit all patients equally, and some still respond either equally to or better than anti-vascular endothelial growth factor alone. This review revealed biomarker modeling that impacts treatment selection. Recent tumor profiling into "angiogenic signature" more sensitive to angiogenic agents versus "immune signature" more likely to achieve the best response with immunotherapy should be validated. Tumor biology features might be more powerful than clinical classification for a tailored treatment approach.
Keywords: Angiogenesis; Biomarkers; Immune check inhibitors; Immunotherapy; Metastases; PD-L1; Renal cell carcinoma; Tyrosine kinase inhibitor.
© 2022 The Authors.
Figures

Similar articles
-
Impact of Clinicopathological Features on Survival in Patients Treated with First-line Immune Checkpoint Inhibitors Plus Tyrosine Kinase Inhibitors for Renal Cell Carcinoma: A Meta-analysis of Randomized Clinical Trials.Eur Urol Focus. 2022 Mar;8(2):514-521. doi: 10.1016/j.euf.2021.03.001. Epub 2021 Mar 11. Eur Urol Focus. 2022. PMID: 33714725 Review.
-
Sequencing and Combination of Systemic Therapy in Metastatic Renal Cell Carcinoma.Eur Urol Oncol. 2019 Sep;2(5):505-514. doi: 10.1016/j.euo.2019.06.022. Epub 2019 Aug 1. Eur Urol Oncol. 2019. PMID: 31377308 Review.
-
Predictive Biomarkers of Response to Immunotherapy in Metastatic Renal Cell Cancer.Front Oncol. 2020 Aug 12;10:1644. doi: 10.3389/fonc.2020.01644. eCollection 2020. Front Oncol. 2020. PMID: 32903369 Free PMC article. Review.
-
The Predictive Value of Programmed Death Ligand 1 in Patients with Metastatic Renal Cell Carcinoma Treated with Immune-checkpoint Inhibitors: A Systematic Review and Meta-analysis.Eur Urol. 2021 Jun;79(6):783-792. doi: 10.1016/j.eururo.2020.10.006. Epub 2020 Nov 7. Eur Urol. 2021. PMID: 33172722
-
Systemic Treatment of Metastatic Clear Cell Renal Cell Carcinoma in 2018: Current Paradigms, Use of Immunotherapy, and Future Directions.Eur Urol. 2019 Jan;75(1):100-110. doi: 10.1016/j.eururo.2018.10.010. Epub 2018 Oct 13. Eur Urol. 2019. PMID: 30327274 Review.
References
-
- Leibovich B.C., Lohse C.M., Crispen P.L., et al. Histological subtype is an independent predictor of outcome for patients with renal cell carcinoma. J Urol. 2010;183:1309–1315. - PubMed
-
- Lipworth L., Morgans A.K., Edwards T.L., et al. Renal cell cancer histological subtype distribution differs by race and sex. BJU Int. 2016;117:260–265. - PubMed
-
- SEER. Cancer of the kidney and renal pelvis—Cancer Stat Facts. https://seer.cancer.gov/statfacts/html/kidrp.html.
-
- Rini B.I., Plimack E.R., Stus V., et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1116–1127. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
