

Human Immunodeficiency Virus Infection-Associated Cardiomyopathy and Heart Failure
- PMID: 36573732
- PMCID: PMC9695202
- DOI: 10.3390/jpm12111760
Human Immunodeficiency Virus Infection-Associated Cardiomyopathy and Heart Failure
Abstract
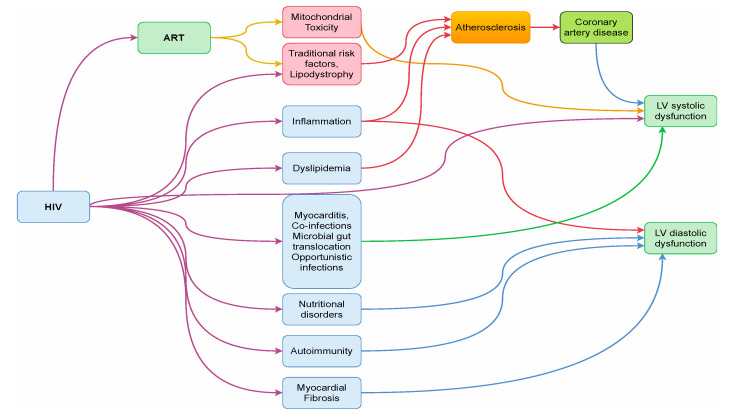
The landscape of human immunodeficiency virus (HIV) epidemiology and treatment is ever-changing, with the widespread and evolving use of antiretroviral therapy (ART). With timely ART, people living with HIV (PLWH) are nearing the life expectancies and the functionality of the general population; nevertheless, the effects of HIV and ART on cardiovascular health remain under investigation. The pathophysiology of HIV-related cardiomyopathy and heart failure (HF) have historically been attributed to systemic inflammation and changes in cardiometabolic function and cardiovascular architecture. Importantly, newer evidence suggests that ART also plays a role in modulating the process of HIV-related cardiomyopathy and HF. In the short term, newer highly active ART (HAART) seems to have cardioprotective effects; however, emerging data on the long-term cardiovascular outcomes of certain HAART medications, i.e., protease inhibitors, raise concerns about the potential adverse effects of these drugs in the clinical course of HIV-related HF. As such, the traditional phenotypes of dilated cardiomyopathy and left ventricular systolic failure that are associated with HIV-related heart disease are incrementally being replaced with increasing rates of diastolic dysfunction and ischemic heart disease. Moreover, recent studies have found important links between HIV-related HF and other clinical and biochemical entities, including depression, which further complicate cardiac care for PLWH. Considering these trends in the era of ART, the traditional paradigms of HIV-related cardiomyopathy and HF are being called into question, as is the therapeutic role of interventions such as ventricular assist devices and heart transplantation. In all, the mechanisms of HIV-related myocardial damage and the optimal approaches to the prevention and the treatment of cardiomyopathy and HF in PLWH remain under investigation.
Keywords: HAART; cardiomyopathy; heart failure; human immunodeficiency virus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Cardiomyopathy and Heart Failure in Patients With HIV Infection.Can J Cardiol. 2019 Mar;35(3):299-309. doi: 10.1016/j.cjca.2018.10.009. Epub 2018 Oct 19. Can J Cardiol. 2019. PMID: 30621958 Review.
-
Cardiac adiposity as a modulator of cardiovascular disease in HIV.HIV Med. 2021 Nov;22(10):879-891. doi: 10.1111/hiv.13166. Epub 2021 Sep 12. HIV Med. 2021. PMID: 34514685 Review.
-
HIV Infection and Risk of Cardiovascular Diseases Beyond Coronary Artery Disease.Curr Atheroscler Rep. 2017 May;19(5):20. doi: 10.1007/s11883-017-0652-3. Curr Atheroscler Rep. 2017. PMID: 28315199 Free PMC article. Review.
-
Dilated cardiomyopathy in two adult human immunodeficiency positive (HIV+) patients possibly related to highly active antiretroviral therapy (HAART).Eur J Med Res. 2005 Sep 12;10(9):395-9. Eur J Med Res. 2005. PMID: 16183552
-
Human immunodeficiency virus-associated heart failure in sub-Saharan Africa: evolution in the epidemiology, pathophysiology, and clinical manifestations in the antiretroviral era.ESC Heart Fail. 2016 Sep;3(3):158-167. doi: 10.1002/ehf2.12087. Epub 2016 Mar 3. ESC Heart Fail. 2016. PMID: 28834662 Free PMC article. Review.
References
-
- Shah A.S., Stelzle D., Lee K.K., Beck E.J., Alam S., Clifford S., Longenecker C.T., Strachan F., Bagchi S., Whiteley W., et al. Global Burden of Atherosclerotic Cardiovascular Disease in People Living with HIV. Circulation. 2018;138:1100–1112. doi: 10.1161/CIRCULATIONAHA.117.033369. - DOI - PMC - PubMed
-
- Remick J., Georgiopoulou V., Marti C., Ofotokun I., Kalogeropoulos A., Lewis W., Butler J. Heart failure in patients with human immunodeficiency virus infection: Epidemiology, pathophysiology, treatment, and future research. Circulation. 2014;129:1781–1789. doi: 10.1161/CIRCULATIONAHA.113.004574. - DOI - PMC - PubMed
-
- Feinstein M.J., Steverson A.B., Ning H., Pawlowski A.E., Schneider D., Ahmad F.S., Sanders J.M., Sinha A., Nance R.M., Achenbach C.J., et al. Adjudicated Heart Failure in HIV-Infected and Uninfected Men and Women. J. Am. Heart Assoc. 2018;7:e009985. doi: 10.1161/JAHA.118.009985. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
