

Added value of semi-quantitative analysis of [18F]FDG PET/CT for the diagnosis of device-related infections in patients with a left ventricular assist device
- PMID: 36573930
- PMCID: PMC10229264
- DOI: 10.1093/ehjci/jeac260
Added value of semi-quantitative analysis of [18F]FDG PET/CT for the diagnosis of device-related infections in patients with a left ventricular assist device
Abstract
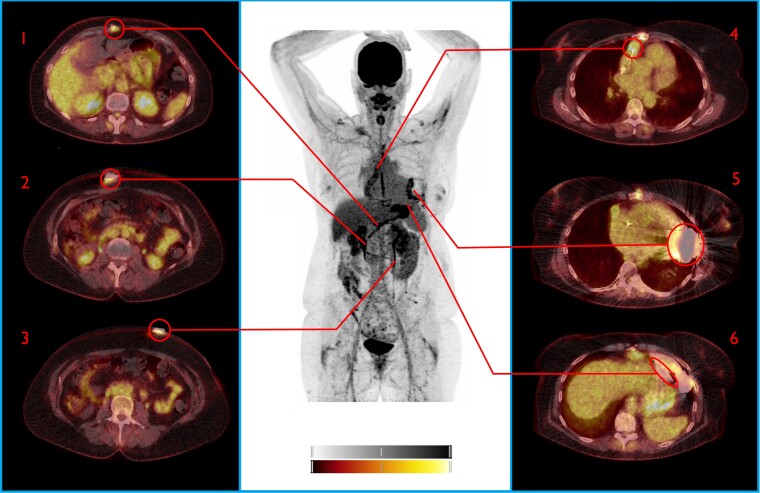
Aims: Left ventricular assist devices (LVADs) improve quality of life and survival in patients with advanced heart failure, but device-related infections (DRIs) remain cumbersome. We evaluated the diagnostic capability of [18F]FDG PET/CT, factors affecting its accuracy, and the additive value of semi-quantitative analysis for the diagnosis of DRI.
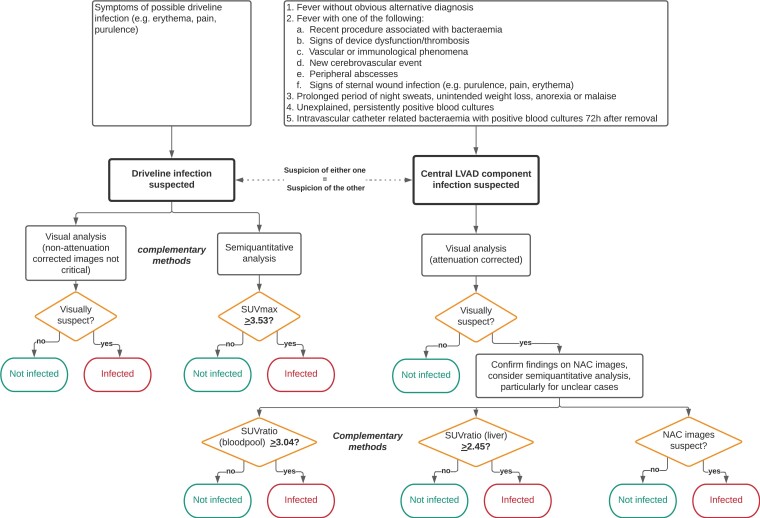
Methods and results: LVAD recipients undergoing [18F]FDG PET/CT between 2012 and 2020 for suspected DRI were retrospectively included. [18F]FDG PET/CT was performed and evaluated in accordance with EANM guidelines. The final diagnosis of DRI, based on multidisciplinary consensus and findings during surgery, whenever performed, was used as the reference for diagnosis. 41 patients were evaluated for 59 episodes of suspected DRI. The clinical evaluation established driveline infection in 32 (55%) episodes, central device infection in 6 (11%), and combined infection in 2 (4%). Visual analysis of [18F]FDG PET/CT achieved a sensitivity and specificity for driveline infections of 0.79 and 0.71, respectively, whereas semi-quantitative analysis achieved a sensitivity and specificity of 0.94 and 0.83, respectively. For central device component infection, visual analysis of [18F]FDG PET/CT achieved a sensitivity and specificity of 0.75 and 0.60, respectively. Semi-quantitative analysis using SUVratio achieved a sensitivity and specificity of 1.0 and 0.8, respectively. The increase of specificity for central component infection was statistically significant (P = 0.05).
Conclusions: [18F]FDG PET/CT reliably predicts the presence of DRI in LVAD recipients. Semi-quantitative analysis may increase the specificity of [18F]FDG PET/CT for the analysis of central device component infection and should be considered in equivocal cases after visual analysis.
Keywords: LVAD; [18F]FDG PET/CT; device-related infection; semi-quantitative analysis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: K.D. reports speaker fees from Abbott, manufacturer of HMII and HM3 LVAD. All other authors declare no potential conflict of interest.
Figures




References
-
- Molina EJ, Shah P, Kiernan MS, Cornwell WK III, Copeland H, Takeda Ket al. . The society of thoracic surgeons intermacs 2020 annual report. Ann Thorac Surg 2021;111:778–92. - PubMed
-
- Kirklin JK, Naftel DC, Pagani FD, Kormos RL, Stevenson LW, Blume EDet al. . Seventh INTERMACS annual report: 15,000 patients and counting. J Heart Lung Transplant [Internet] 2015;34:1495–504. - PubMed
-
- Aggarwal A, Gupta A, Kumar S, Baumblatt JA, Pauwaa S, Gallagher Cet al. . Are blood stream infections associated with an increased risk of hemorrhagic stroke in patients with a left ventricular assist device? ASAIO J 2012;58:509–13. - PubMed
-
- Trachtenberg BH, Cordero-Reyes AM, Aldeiri M, Alvarez P, Bhimaraj A, Ashrith Get al. . Persistent blood stream infection in patients supported with a continuous-flow left ventricular assist device is associated with an increased risk of cerebrovascular accidents. J Card Fail [Internet] 2015;21:119–25. - PubMed
-
- Lesicka A, Feinman JW, Thiele K, Andrawes MN. Echocardiographic artifact induced by HeartWare left ventricular assist device. Anesth Analg 2015;120:1208–11. - PubMed
