

Exome Sequencing of a Clinical Population for Autosomal Dominant Polycystic Kidney Disease
- PMID: 36573973
- PMCID: PMC9856880
- DOI: 10.1001/jama.2022.22847
Exome Sequencing of a Clinical Population for Autosomal Dominant Polycystic Kidney Disease
Abstract
Importance: Most studies of autosomal dominant polycystic kidney disease (ADPKD) genetics have used kidney specialty cohorts, focusing on PKD1 and PKD2. These can lead to biased estimates of population prevalence of ADPKD-associated gene variants and their phenotypic expression.
Objective: To determine the prevalence of ADPKD and contributions of PKD1, PKD2, and other genes related to cystic kidney disease in a large, unselected cohort.
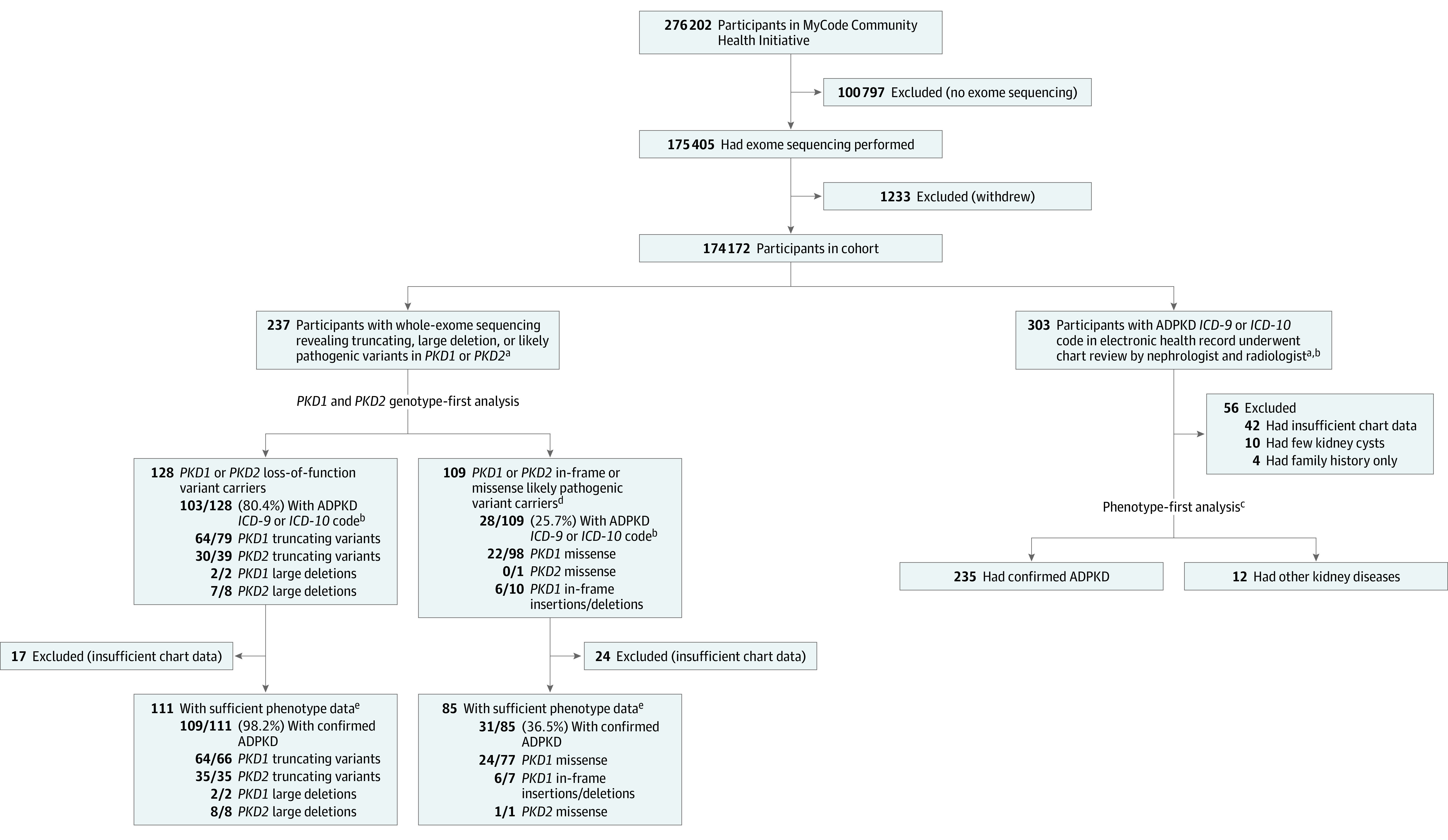
Design, setting, and participants: This retrospective observational study used an unselected health system-based cohort in central and northeast Pennsylvania with exome sequencing (enrolled from 2004 to 2020) and electronic health record data (up to October 2021). The genotype-first approach included the entire cohort and the phenotype-first approach focused on patients with ADPKD diagnosis codes, confirmed by chart and imaging review.
Exposures: Loss-of-function (LOF) variants in PKD1, PKD2, and other genes associated with cystic kidney disease (ie, ALG8, ALG9, DNAJB11, GANAB, HNF1B, IFT140, SEC61B, PKHD1, PRKCSH, SEC63); likely pathogenic missense variants in PKD1 and PKD2.
Main outcomes and measures: Genotype-first analysis: ADPKD diagnosis code (Q61.2, Q61.3, 753.13, 753.12); phenotype-first analysis: presence of a rare variant in PKD1, PKD2, or other genes associated with cystic kidney disease.
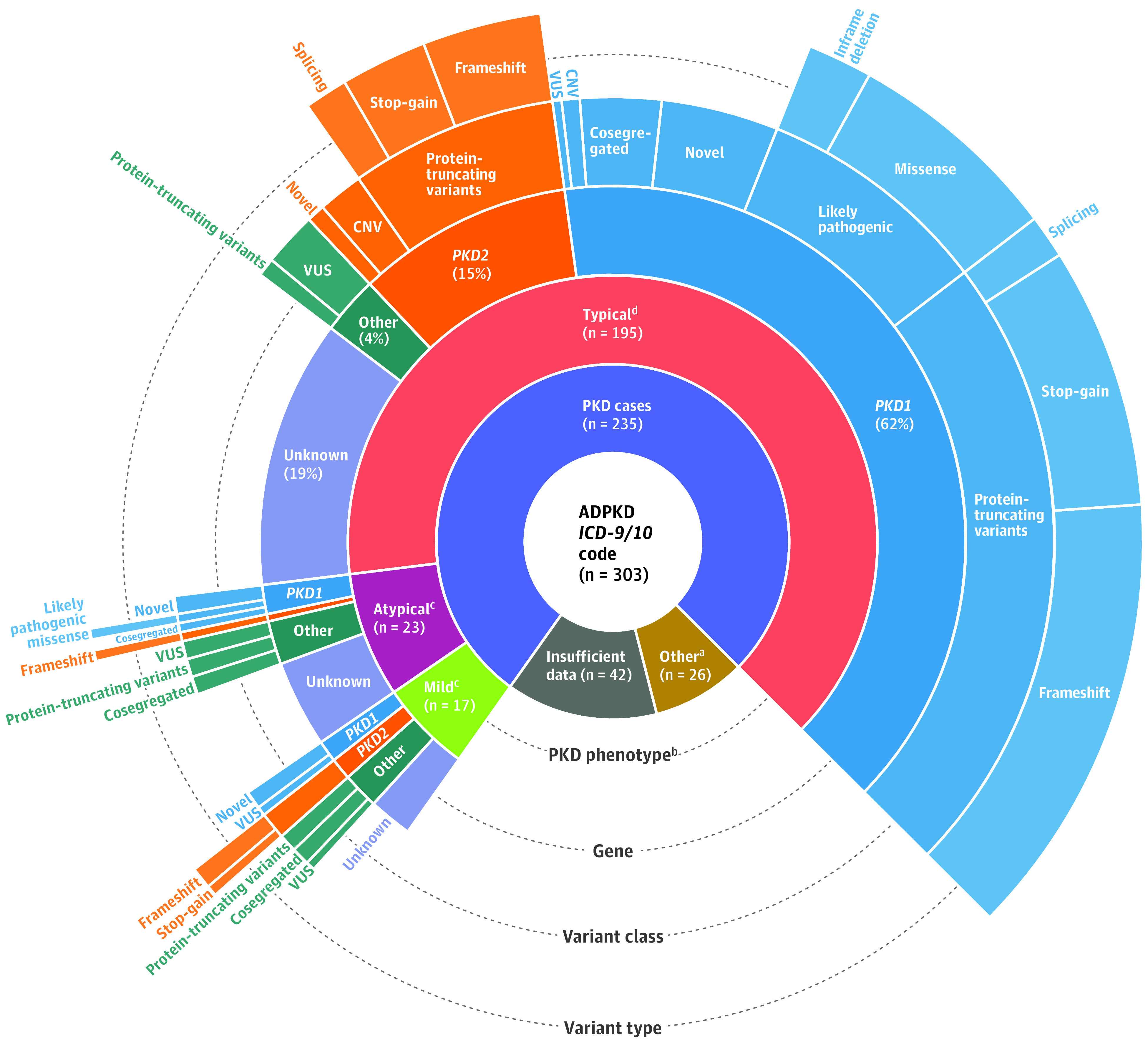
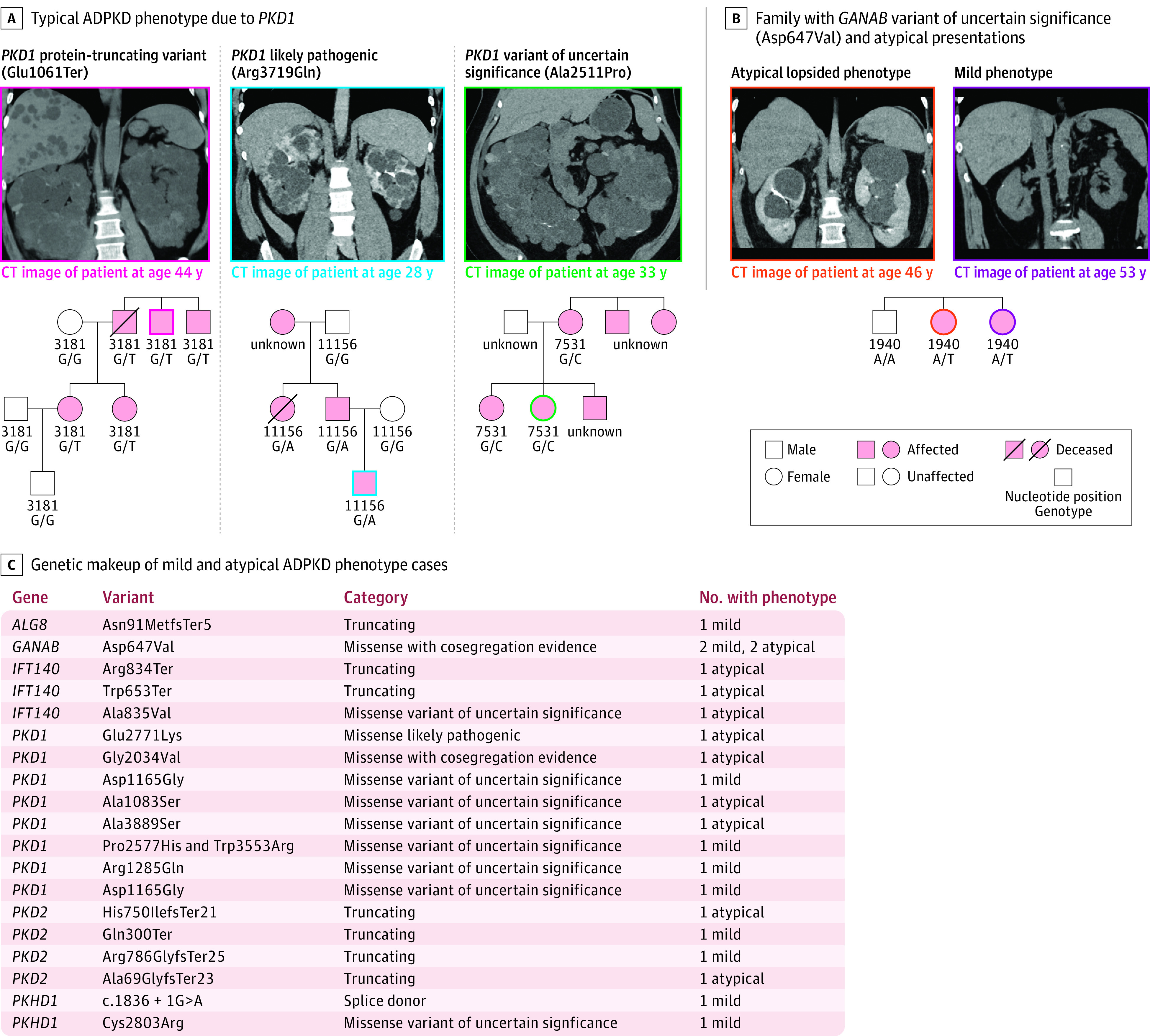
Results: Of 174 172 patients (median age, 60 years; 60.6% female; 93% of European ancestry), 303 patients had ADPKD diagnosis codes, including 235 with sufficient chart review data for confirmation. In addition to PKD1 and PKD2, LOF variants in IFT140, GANAB, and HNF1B were associated with ADPKD diagnosis after correction for multiple comparisons. Among patients with LOF variants in PKD1, 66 of 68 (97%) had ADPKD; 43 of 43 patients (100%) with LOF variants in PKD2 had ADPKD. In contrast, only 24 of 77 patients (31.2%) with a PKD1 missense variant previously classified as "likely pathogenic" had ADPKD, suggesting misclassification or variable penetrance. Among patients with ADPKD diagnosis confirmed by chart review, 180 of 235 (76.6%) had a potential genetic cause, with the majority being rare variants in PKD1 (127 patients) or PKD2 (34 patients); 19 of 235 (8.1%) had variants in other genes associated with cystic kidney disease. Of these 235 patients with confirmed ADPKD, 150 (63.8%) had a family history of ADPKD. The yield for a genetic determinant of ADPKD was higher for those with a family history of ADPKD compared with those without family history (91.3% [137/150] vs 50.6% [43/85]; difference, 40.7% [95% CI, 29.2%-52.3%]; P < .001). Previously unreported PKD1, PKD2, and GANAB variants were identified with pedigree data suggesting pathogenicity, and several PKD1 missense variants previously reported as likely pathogenic appeared to be benign.
Conclusions and relevance: This study demonstrates substantial genetic and phenotypic variability in ADPKD among patients within a regional health system in the US.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
