

Nonsteroidal anti-inflammatory drugs as a targeted therapy for bone marrow failure in Ghosal hematodiaphyseal dysplasia
- PMID: 36574346
- PMCID: PMC10082374
- DOI: 10.1182/blood.2022018667
Nonsteroidal anti-inflammatory drugs as a targeted therapy for bone marrow failure in Ghosal hematodiaphyseal dysplasia
Abstract
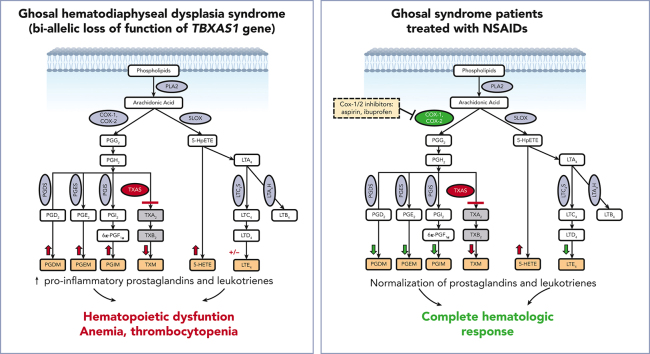
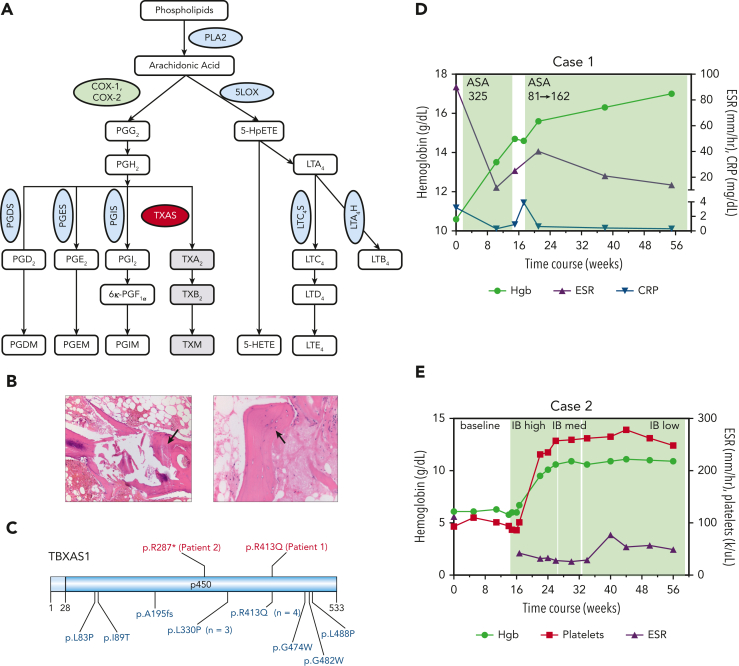
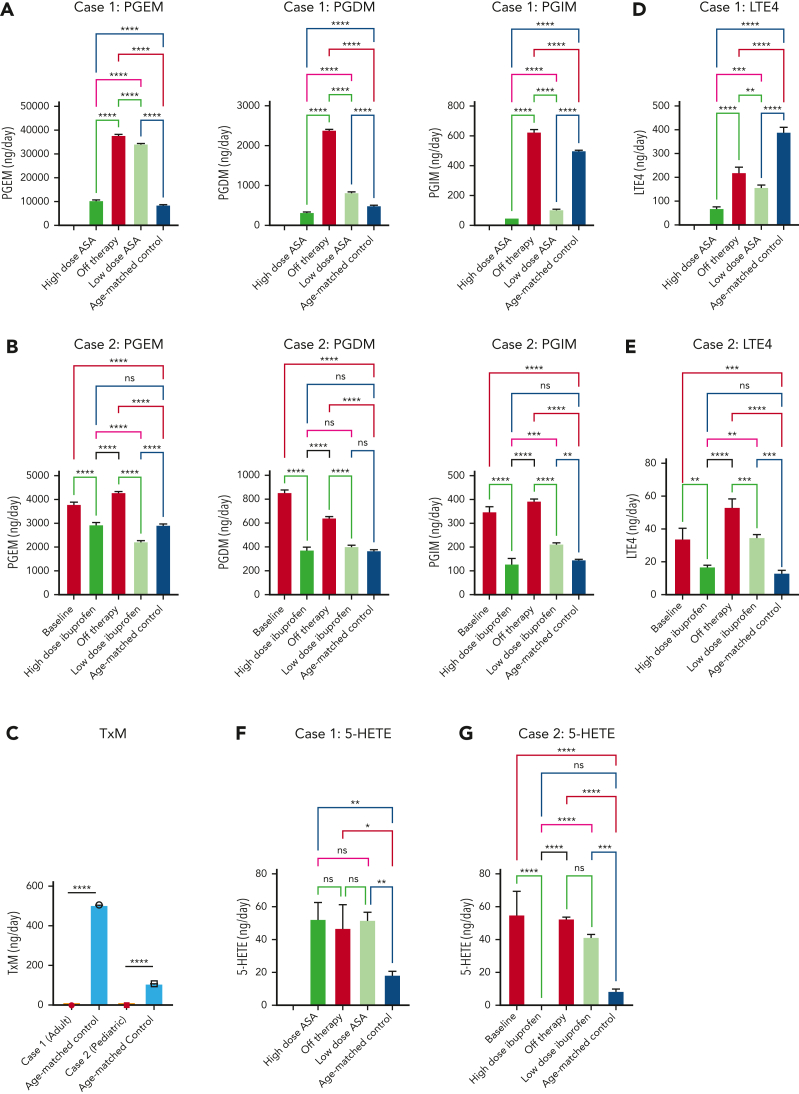
Advances in genomic diagnostics hold promise for improved care of rare hematologic diseases. Here, we describe a novel targeted therapeutic approach for Ghosal hematodiaphyseal dysplasia, an autosomal recessive disease characterized by severe normocytic anemia and bone abnormalities due to loss-of-function mutations in thromboxane A synthase 1 (TBXAS1). TBXAS1 metabolizes prostaglandin H2 (PGH2), a cyclooxygenase (COX) product of arachidonic acid, into thromboxane A2. Loss-of-function mutations in TBXAS result in an increase in PGH2 availability for other PG synthases. The current treatment for Ghosal hematodiaphyseal dysplasia syndrome consists of corticosteroids. We hypothesize that nonsteroidal anti-inflammatory drugs (NSAIDs), which inhibit COX-1 and COX-2, could ameliorate the effects of TBXAS1 loss and improve hematologic function by reducing prostaglandin formation. We treated 2 patients with Ghosal hematodiaphyseal dysplasia syndrome, an adult and a child, with standard doses of NSAIDs (aspirin or ibuprofen). Both patients had rapid improvements concerning hematologic parameters and inflammatory markers without adverse events. Mass spectrometry analysis demonstrated that urinary PG metabolites were increased along with proinflammatory lipoxygenase (LOX) products 5-hydroxyeicosatetraenoic acid and leukotriene E4. Our data show that NSAIDs at standard doses surprisingly reduced both COX and LOX products, leading to the resolution of cytopenia, and should be considered for first-line treatment for Ghosal hematodiaphyseal dysplasia syndrome.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures

Comment in
-
Blocking COX unlocks response in GHDD.Blood. 2023 Mar 30;141(13):1497-1498. doi: 10.1182/blood.2022019351. Blood. 2023. PMID: 36995703 No abstract available.
References
-
- Ghosal SP, Mukherjee AK, Mukherjee D, Ghosh AK. Diaphyseal dysplasia associated with anemia. J Pediatr. 1988;113(1):49–57. - PubMed
-
- Geneviève D, Proulle V, Isidor B, et al. Thromboxane synthase mutations in an increased bone density disorder (Ghosal syndrome) Nat Genet. 2008;40(3):284–286. - PubMed
-
- Joy P, Yoganathan S, Korula S, et al. Ghosal hematodiaphyseal dysplasia and response to corticosteroid therapy. Am J Med Genet. 2021;185(2):596–599. - PubMed
-
- Arora R, Aggarwal S, Deme S. Ghosal hematodiaphyseal dysplasia—a concise review including an illustrative patient. Skeletal Radiol. 2015;44(3):447–450. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
