

The ectonucleotidase CD39 identifies tumor-reactive CD8+ T cells predictive of immune checkpoint blockade efficacy in human lung cancer
- PMID: 36574773
- PMCID: PMC9887636
- DOI: 10.1016/j.immuni.2022.12.001
The ectonucleotidase CD39 identifies tumor-reactive CD8+ T cells predictive of immune checkpoint blockade efficacy in human lung cancer
Abstract
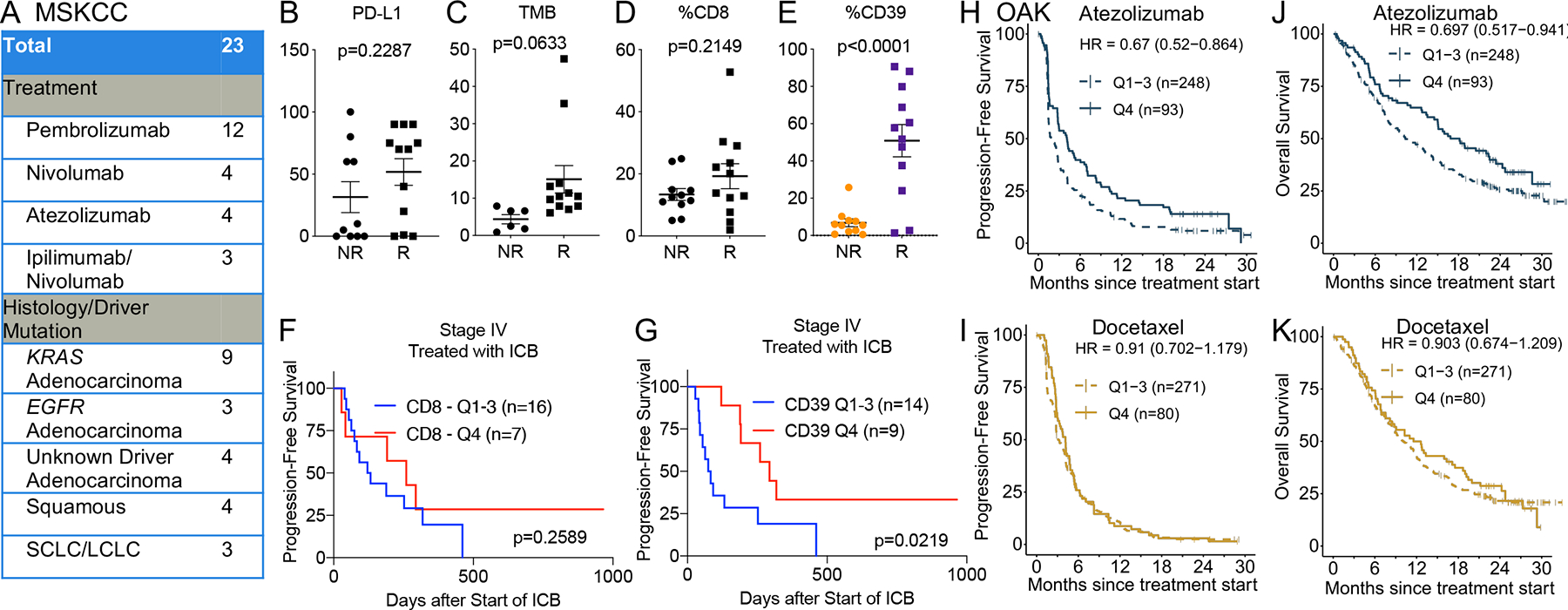
Improved identification of anti-tumor T cells is needed to advance cancer immunotherapies. CD39 expression is a promising surrogate of tumor-reactive CD8+ T cells. Here, we comprehensively profiled CD39 expression in human lung cancer. CD39 expression enriched for CD8+ T cells with features of exhaustion, tumor reactivity, and clonal expansion. Flow cytometry of 440 lung cancer biospecimens revealed weak association between CD39+ CD8+ T cells and tumoral features, such as programmed death-ligand 1 (PD-L1), tumor mutation burden, and driver mutations. Immune checkpoint blockade (ICB), but not cytotoxic chemotherapy, increased intratumoral CD39+ CD8+ T cells. Higher baseline frequency of CD39+ CD8+ T cells conferred improved clinical outcomes from ICB therapy. Furthermore, a gene signature of CD39+ CD8+ T cells predicted benefit from ICB, but not chemotherapy, in a phase III clinical trial of non-small cell lung cancer. These findings highlight CD39 as a proxy of tumor-reactive CD8+ T cells in human lung cancer.
Keywords: CD8(+) T cells; T cell receptors; immune checkpoint blockade; non-small cell lung cancer; tumor mutation burden.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests C.A.K. received research funding support from Kite/Gilead and Intima Bioscience; is on the Scientific and/or Clinical Advisory Boards of Achilles Therapeutics, Aleta BioTherapeutics, Bellicum Pharmaceuticals, Catamaran Bio, Obsidian Therapeutics, and T-knife; and has performed consulting services for Bristol Myers Squibb, PACT Pharma, and Roche/Genentech. C.A.K. is a co-inventor on patent applications related to TCRs targeting public neoantigens unrelated to the current work. M.D.H. received a research grant from BMS; personal fees from Achilles, Arcus, AstraZeneca, Blueprint, BMS, Genentech/Roche, Genzyme, Immunai, Instil Bio, Janssen, Merck, Mirati, Natera, Nektar, Pact Pharma, Regeneron, Shattuck Labs, and Syndax; and equity options from Arcus, Factorial, Immunai, and Shattuck Labs. A patent filed by MSKCC related to the use of tumor mutational burden to predict response to immunotherapy (PCT/US2015/062208) is pending and licensed by PGDx. J.D.W. is a consultant for Amgen, Apricity, Ascentage Pharma, Astellas, AstraZeneca, Bicara Therapeutics, Boehringer Ingelheim, Bristol Myers Squibb, CellCarta, Chugai, Daiichi Sankyo, Dragonfly, Georgiamune, Idera, Imvaq, Larkspur, Maverick Therapeutics, Merck, Psioxus, Recepta, Tizona, Trishula, Sellas, Surface Oncology, and Werewolf Therapeutics. J.D.W. receives grant/research support from Bristol Myers Squibb and Sephora. J.D.W. has equity in Apricity, Arsenal IO, Ascentage, Beigene, Imvaq, Linneaus, Georgiamune, Maverick, Tizona Pharmaceuticals, and Trieza. J.D.W. is a co-inventor on the following patent application: xenogeneic (canine) DNA vaccines, myeloid-derived suppressor cell (MDSC) assay, anti-PD1 antibody, anti-CTLA4 antibodies, anti-GITR antibodies and methods of use thereof, Newcastle disease viruses for cancer therapy, and prediction of responsiveness to treatment with immunomodulatory therapeutics and method of monitoring abscopal effects during such treatment. J.D.W. and T.M. are co-inventors on patent applications related to CD40 and in situ vaccination (PCT/US2016/045970). T.M. is a consultant for Immunos Therapeutics and Pfizer. T.M. is a cofounder of and equity holder in IMVAQ Therapeutics. T.M. receives research funding from Bristol Myers Squibb, Surface Oncology, Kyn Therapeutics, Infinity Pharmaceuticals, Peregrine Pharmaceuticals, Adaptive Biotechnologies, Leap Therapeutics, and Aprea Therapeutics. T.M. is an inventor on patent applications related to work on oncolytic viral therapy, alpha virus-based vaccine, neoantigen modeling, CD40, GITR, OX40, PD-1, and CTLA-4. C.M.R. has consulted regarding oncology drug development with AbbVie, Amgen, Ascentage, AstraZeneca, BMS, Celgene, Daiichi Sankyo, Genentech/Roche, Ipsen, Loxo, and PharmaMar and is on the scientific advisory boards of Elucida, Bridge, and Harpoon. B.Y.N. and X.G. are employees and stockholders of Genentech/Roche.
Figures





References
-
- Thommen DS, Koelzer VH, Herzig P, Roller A, Trefny M, Dimeloe S, Kiialainen A, Hanhart J, Schill C, Hess C, et al. (2018). A transcriptionally and functionally distinct PD-1(+) CD8(+) T cell pool with predictive potential in non-small-cell lung cancer treated with PD-1 blockade. Nat Med 24, 994–1004. 10.1038/s41591-018-0057-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
