

Placental telomere length shortening is not associated with severe preeclampsia but the gestational age
- PMID: 36575046
- PMCID: PMC9925682
- DOI: 10.18632/aging.204445
Placental telomere length shortening is not associated with severe preeclampsia but the gestational age
Abstract
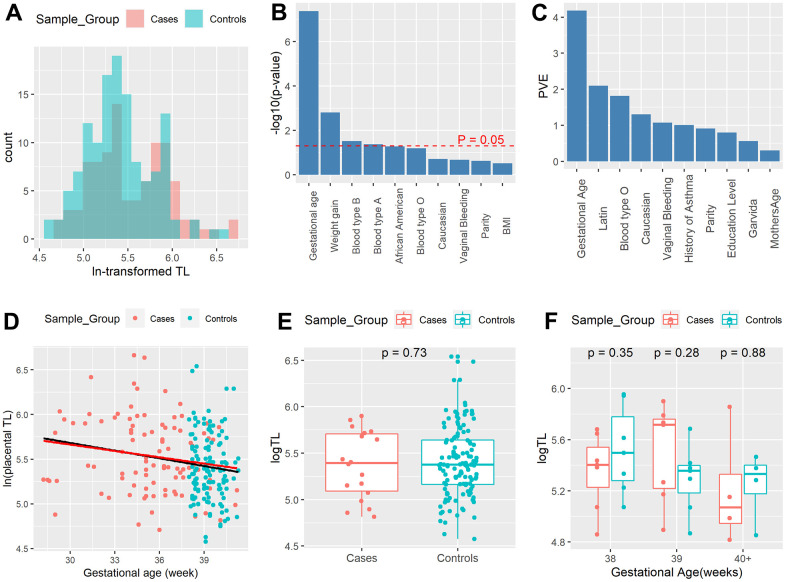
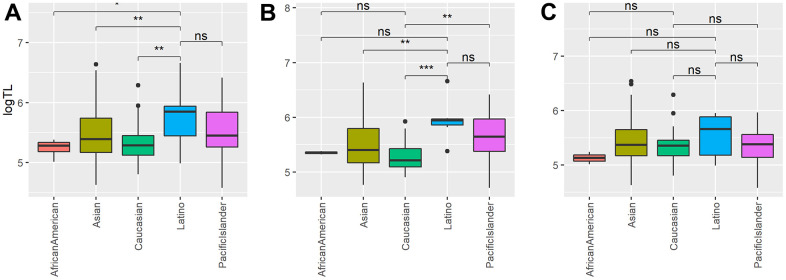
Variations in telomere length (TL) have been associated with aging, stress, and many diseases. Placenta TL is an essential molecular component influencing the outcome of birth. Previous investigations into the relationship between placenta TL and preeclampsia (PE) have produced conflicting findings. We conducted a retrospective case-control analysis in this study to address the disparity. We used placenta samples from 224 births received from Hawaii Biorepository (HiBR) between 2006 and 2013, comprising 129 healthy full-term controls and 95 severe PE samples. The average absolute placental TL was calculated using the quantitative polymerase chain reaction (qPCR) technique. We utilized multiple linear regressions to associate placental TL with severe PE and other demographic, clinical and physiological data. The outcome demonstrates that the placental TL of severe PE cases did not significantly differ from that of healthy controls. Instead, there is a strong correlation between gestational age and placenta TL shortening. Placental TL also exhibits racial differences: (1) Latino moms' TL is significantly longer than non-Latino mothers' (p=0.009). (2) Caucasian patients with severe PE have shorter TL than non-Caucasian patients (p=0.0037). This work puts the long-standing question of whether severe PE influences placental TL to rest. Placental TL is not related to severe PE but is negatively associated with gestational age and is also affected by race.
Keywords: placenta; placenta aging; preeclampsia; pregnancy; telomere length.
Conflict of interest statement
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
