

Emerging molecular imaging targets and tools for myocardial fibrosis detection
- PMID: 36575058
- PMCID: PMC9936837
- DOI: 10.1093/ehjci/jeac242
Emerging molecular imaging targets and tools for myocardial fibrosis detection
Abstract
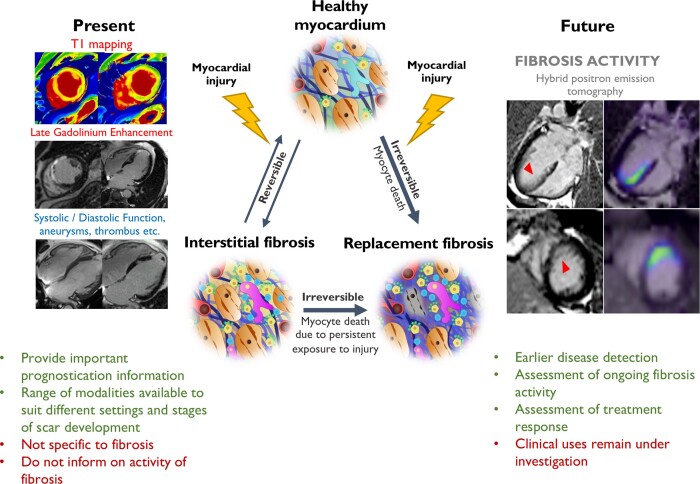
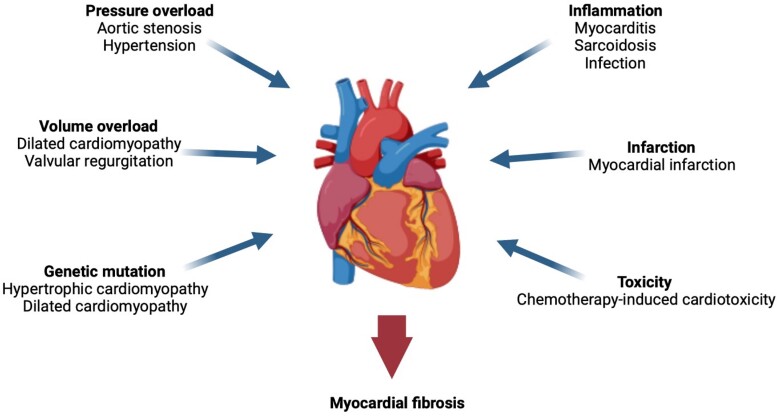
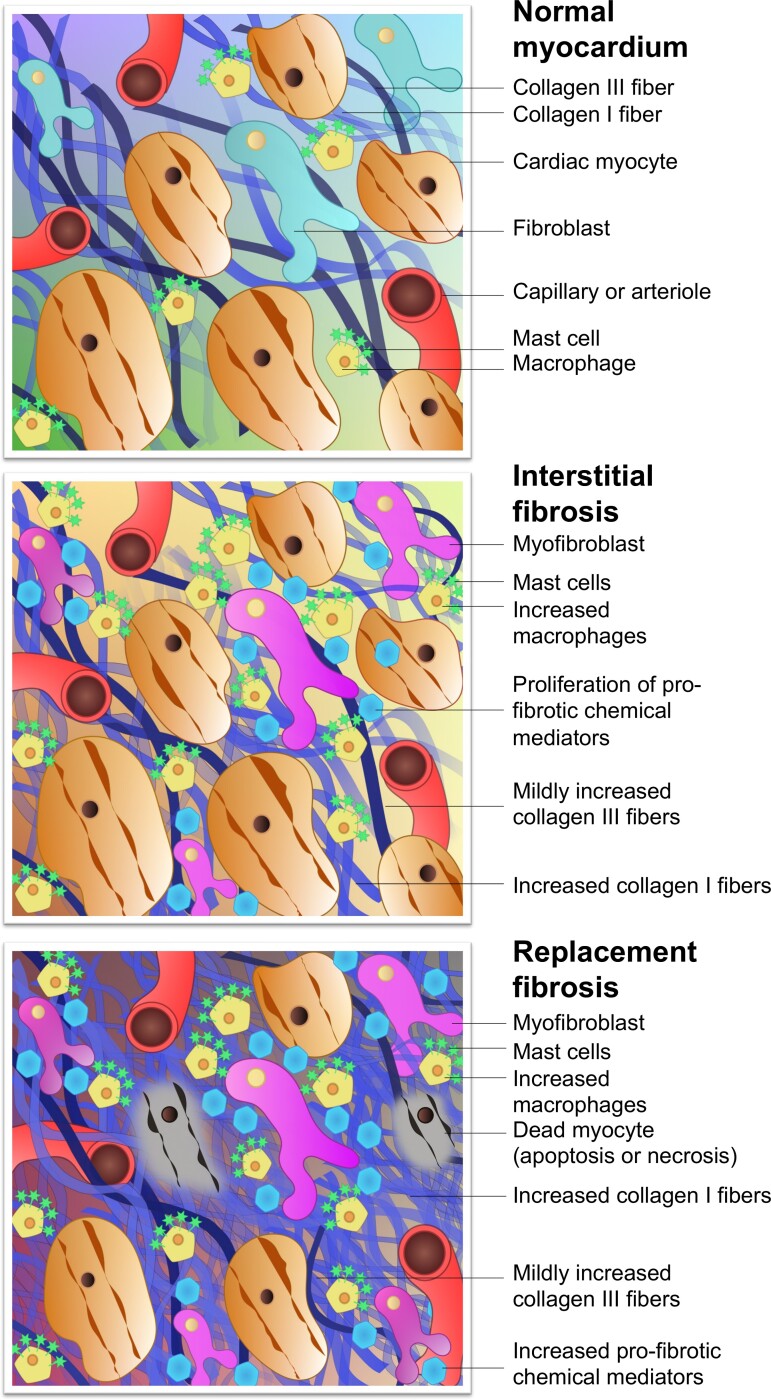
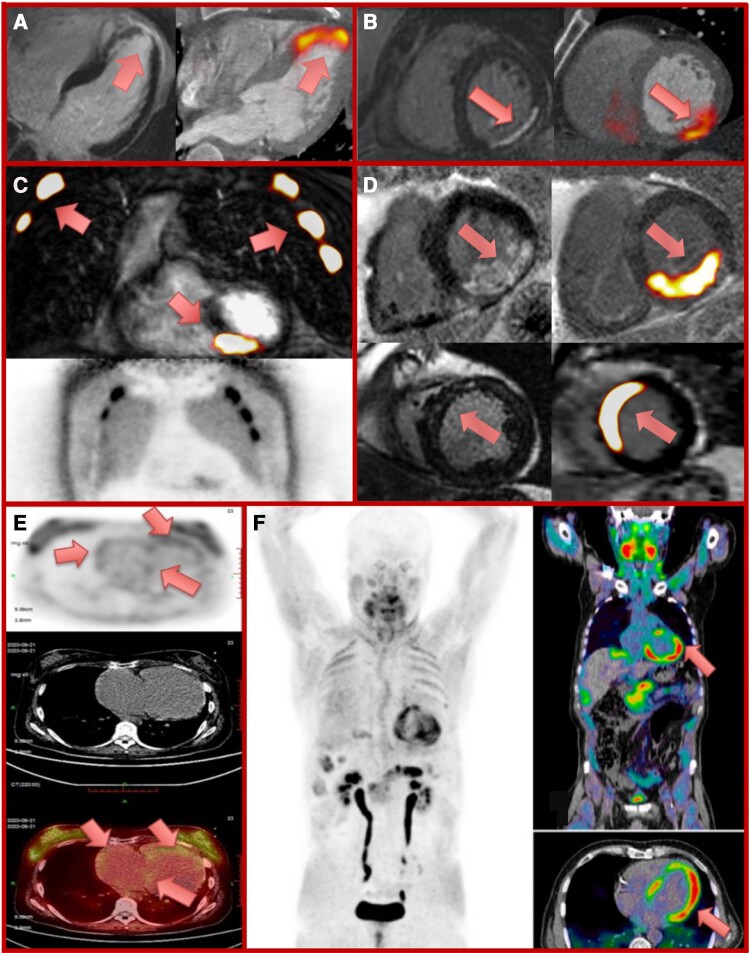
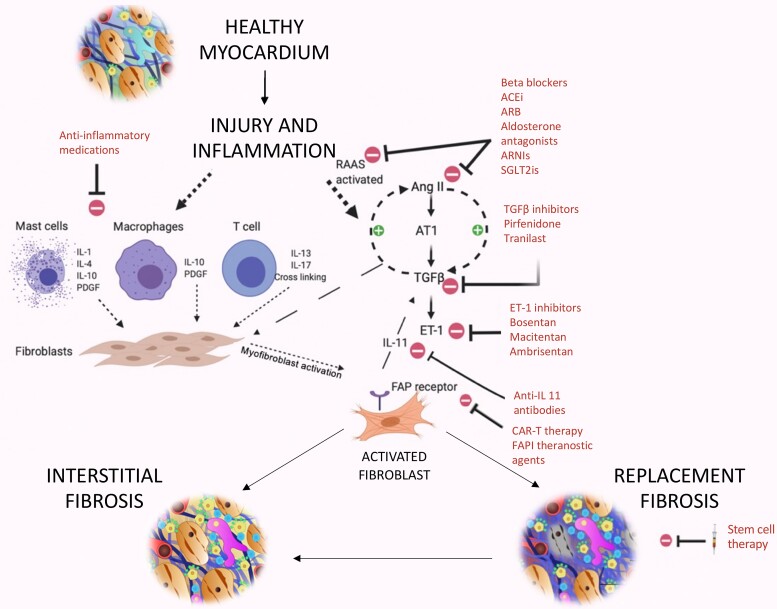
Myocardial fibrosis is the heart's common healing response to injury. While initially seeking to optimize the strength of diseased tissue, fibrosis can become maladaptive, producing stiff poorly functioning and pro-arrhythmic myocardium. Different patterns of fibrosis are associated with different myocardial disease states, but the presence and quantity of fibrosis largely confer adverse prognosis. Current imaging techniques can assess the extent and pattern of myocardial scarring, but lack specificity and detect the presence of established fibrosis when the window to modify this process may have ended. For the first time, novel molecular imaging methods, including gallium-68 (68Ga)-fibroblast activation protein inhibitor positron emission tomography (68Ga-FAPI PET), may permit highly specific imaging of fibrosis activity. These approaches may facilitate earlier fibrosis detection, differentiation of active vs. end-stage disease, and assessment of both disease progression and treatment-response thereby improving patient care and clinical outcomes.
Keywords: fibroblast activation protein inhibitor; fibrosis imaging; molecular fibrosis imaging; myocardial fibrosis; positron emission tomography and cardiovascular magnetic resonance.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Nagaraju C, Robinson E, Abdesselem M, Trenson S, Dries E, Gilbert Get al. Myofibroblast phenotype and reversibility of fibrosis in patients with end-stage heart failure. J Am Coll Cardiol 2019;73:2267–82. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
