

Sex differences among patients with transthyretin amyloid cardiomyopathy - from diagnosis to prognosis
- PMID: 36575133
- PMCID: PMC10087683
- DOI: 10.1002/ejhf.2646
Sex differences among patients with transthyretin amyloid cardiomyopathy - from diagnosis to prognosis
Abstract
Aims: Transthyretin amyloid cardiomyopathy (ATTR-CM) is predominantly diagnosed in men. The few available studies suggest affected women have a more favourable cardiac phenotype. We aimed to characterize sex differences among consecutive patients with non-hereditary and two prevalent forms of hereditary (h)ATTR-CM diagnosed over a 20-year period.
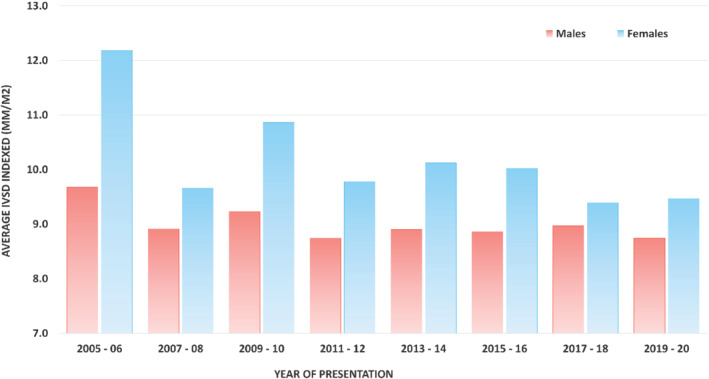
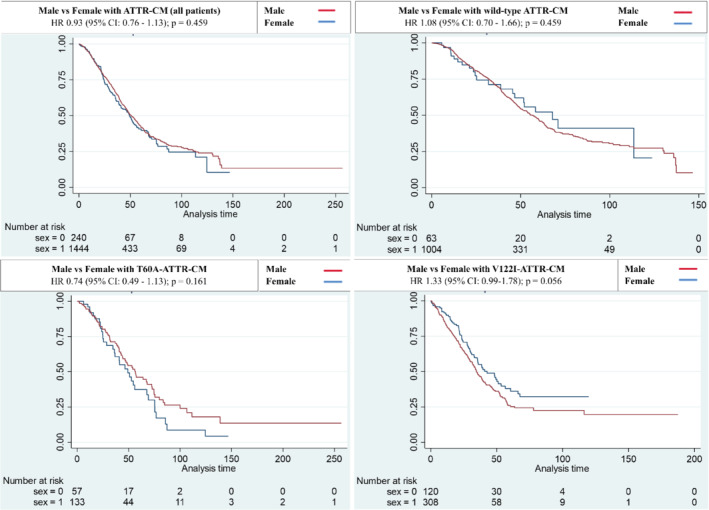
Methods and results: Analysis of deep phenotyping at presentation, changes on serial echocardiography and overall prognosis were evaluated. In total, 1732 consecutive patients were studied, comprising: 1095 with wild-type (wt)ATTR-CM; 206 with T60A-hATTR-CM; and 431 with V122I-hATTR-CM. Female prevalence was greater in T60A-hATTR-CM (29.6%) and V122I-hATTR-CM (27.8%) compared to wtATTR-CM (6%). At presentation, females were 3.3 years older than males (wtATTR-CM: 81.9 vs. 77.8 years; T60A-hATTR-CM: 68.7 vs. 65.1 years; V122I-hATTR-CM: 77.1 vs. 74.9 years). Body size significantly influenced measures of disease severity; when indexed, overall structural and functional phenotype was similar between sexes, the few significant differences suggested a mildly worse phenotype in females. No significant differences were observed in both disease progression on serial echocardiography and mortality across the overall population (p = 0.459) and when divided by genotype (wtATTR-CM: p = 0.730; T60A-hATTR-CM: p = 0.161; V122I-hATTR-CM: p = 0.056).
Conclusion: This study of a well-characterized large cohort of ATTR-CM patients did not demonstrate overall differences between sexes in either clinical phenotype, when indexed, or with respect to disease progression and prognosis. Non-indexed wall thickness measurements may have contributed to both under-representation and delays in diagnosis for affected females and highlights the potential role of utilizing indexed echocardiographic parameters for a more accurate assessment of patients at diagnosis and for disease prognostication.
Keywords: Amyloidosis; Diagnosis; Echocardiography; Prognosis; Sex.
© 2022 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures

Comment in
-
Unravelling the role of sex in the pathophysiology, phenotypic expression and diagnosis of cardiac amyloidosis.Eur J Heart Fail. 2022 Dec;24(12):2364-2366. doi: 10.1002/ejhf.2674. Epub 2022 Sep 15. Eur J Heart Fail. 2022. PMID: 36059061
References
-
- Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. Lancet. 2016;387:2641–54. - PubMed
-
- Fontana M, Ćorović A, Scully P, Moon JC. Myocardial amyloidosis: the exemplar interstitial disease. JACC Cardiovasc Imaging. 2019;12:2345–56. - PubMed
-
- González‐López E, Gagliardi C, Dominguez F, Quarta CC, de Haro‐Del Moral FJ, Milandri A, et al. Clinical characteristics of wild‐type transthyretin cardiac amyloidosis: disproving myths. Eur Heart J. 2017;38:1895–904. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
