

Frequency of thoracic recurrence based on pathological features in patients with ovarian epithelial tumors in stage I versus higher stages
- PMID: 36575285
- PMCID: PMC10147781
- DOI: 10.1007/s11604-022-01374-y
Frequency of thoracic recurrence based on pathological features in patients with ovarian epithelial tumors in stage I versus higher stages
Abstract
Purpose: The aim of this study was to clarify the frequency of thoracic recurrence and identify associated pathological features in postoperative patients with borderline or malignant ovarian epithelial tumors (BMOT) in stage I versus higher stages.
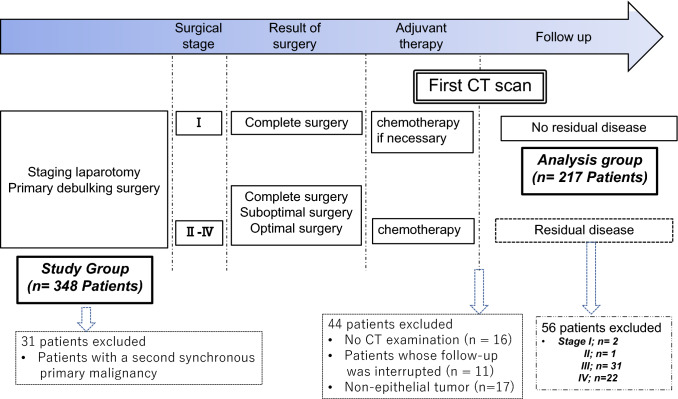
Materials and methods: A total of 368 consecutive patients with a single primary BMOT were treated at our hospital. This study included the 217 patients with no residual disease on the first CT after standard treatment. The timing and pattern of recurrence on follow-up CT images with a scan range from chest to pelvis were evaluated retrospectively. Patient characteristics, tumor histology, and stage were recorded from electronic medical records.
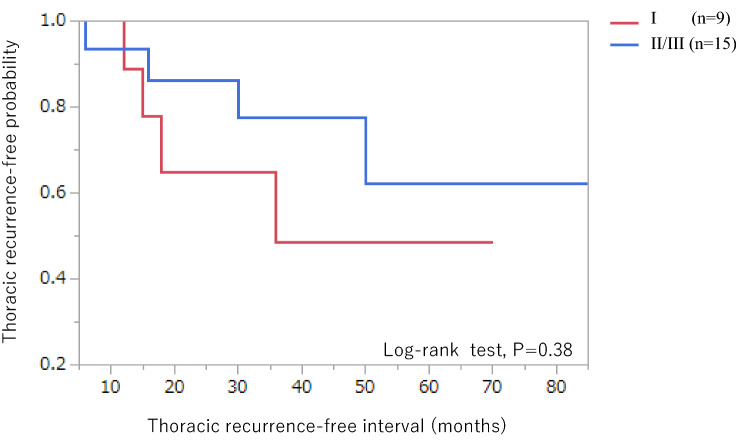
Results: After a median follow-up period of 48 months, recurrence was detected by CT in 9 patients in stage I (n = 159) and 15 in stage II/III (n = 58) (p = 0.0001). Thoracic recurrence was detected in four patients in stage I and four in stage II/III (p = 0.15). Abdominal recurrence was identified as a factor associated with thoracic recurrence (P < 0.001). Clear cell carcinomas accounted for three out of four thoracic recurrences in stage I and two out of four in stage II/III, and had the highest rates of thoracic recurrence (7.7% in stage I and 22.2% in stage II/III) among all histological types associated with thoracic recurrence. Among patients with recurrence, thoracic recurrence-free probability (p = 0.38), median abdominal recurrence-free interval (18 vs 16 months; p = 0.55) and thoracic recurrence-free interval (16.5 vs 23 months; p = 0.89) did not differ significantly between stage I and stage II/III.
Conclusion: The frequency and timing of thoracic recurrence did not differ significantly in postoperative patients with BMOT in stage I versus stage II/III. Abdominal recurrence and a histological type of clear cell carcinoma were most often associated with thoracic recurrence in stage I.
Keywords: CT; Chest recurrence; Follow-up; Ovarian cancer; Stage I.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
