

Non-invasive pediatric cardiac imaging-current status and further perspectives
- PMID: 36575291
- PMCID: PMC9794482
- DOI: 10.1186/s40348-022-00153-z
Non-invasive pediatric cardiac imaging-current status and further perspectives
Abstract
Background: Non-invasive cardiac imaging has a growing role in diagnosis, differential diagnosis, therapy planning, and follow-up in children and adolescents with congenital and acquired cardiac diseases. This review is based on a systematic analysis of international peer-reviewed articles and additionally presents own clinical experiences. It provides an overview of technical advances, emerging clinical applications, and the aspect of artificial intelligence.
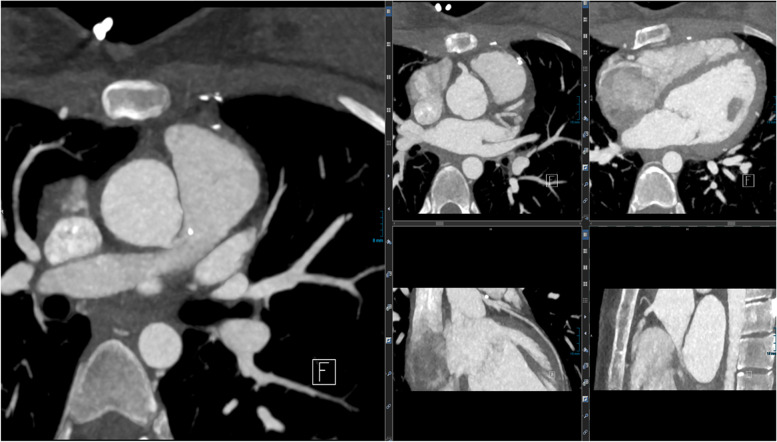
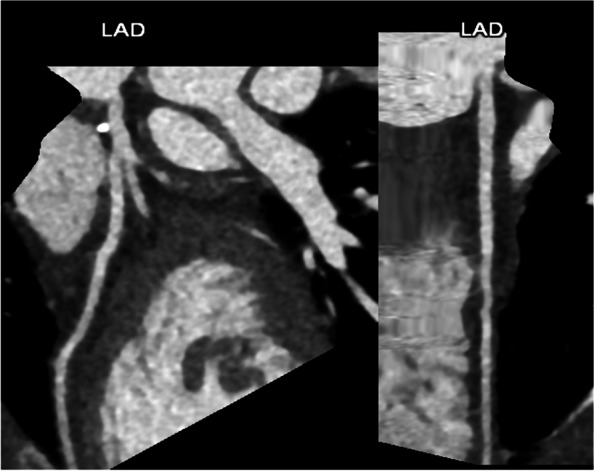
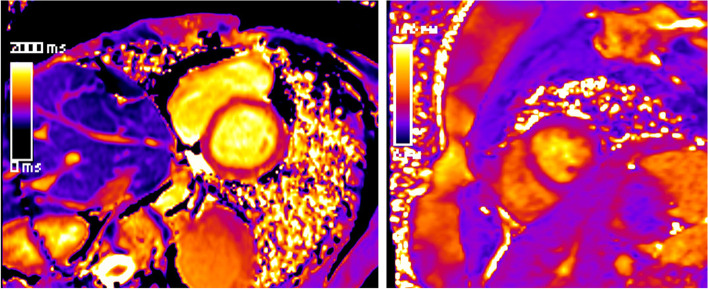
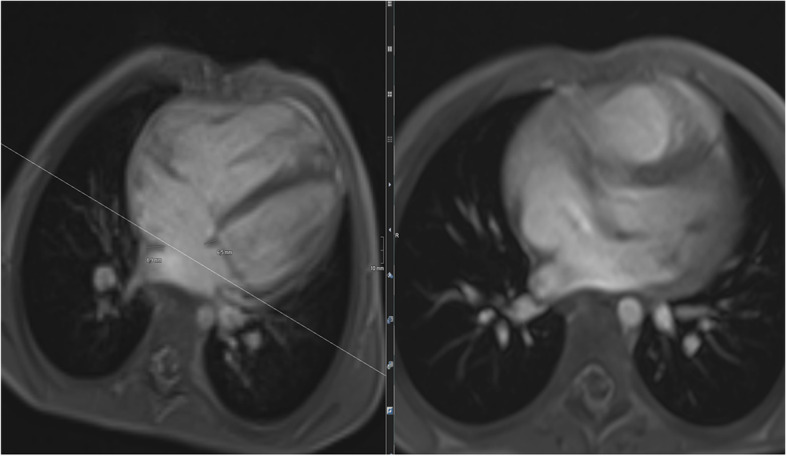
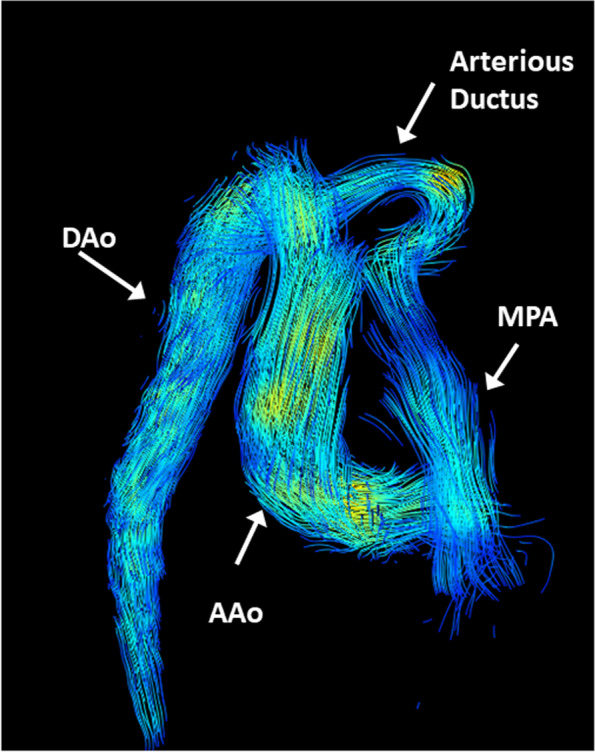
Main body: The main imaging modalities are echocardiography, CT, and MRI. For echocardiography, strain imaging allows a novel non-invasive assessment of tissue integrity, 3D imaging rapid holistic overviews of anatomy. Fast cardiac CT imaging new techniques-especially for coronary assessment as the main clinical indication-have significantly improved spatial and temporal resolution in adjunct with a major reduction in ionizing dose. For cardiac MRI, assessment of tissue integrity even without contrast agent application by mapping sequences is a major technical breakthrough. Fetal cardiac MRI is an emerging technology, which allows structural and functional assessment of fetal hearts including even 4D flow analyses. Last but not least, artificial intelligence will play an important role for improvements of data acquisition and interpretation in the near future.
Conclusion: Non-invasive cardiac imaging plays an integral part in the workup of children with heart disease. In recent years, its main application congenital heart disease has been widened for acquired cardiac diseases.
Keywords: Artificial intelligence; Cardiac CT and MRI; Children and adolescents; Congenital heart disease; Echocardiography; Fetal cardiac MRI; Myocarditis; Non-invasive cardiac imaging; Pediatric cardio-oncology; Recent advances.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures







References
-
- von Scheidt F, Kiesler V, Kaestner M, et al. Left ventricular strain and strain rate during submaximal semisupine bicycle exercise stress echocardiography in healthy adolescents and young adults – systematic protocol and reference values. J Am Soc Echocardiogr. 2020;33:848–857.e1. doi: 10.1016/j.echo.2019.12.015. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
