

Ablation versus anti-arrhythmic therapy for reducing all hospital episodes from recurrent atrial fibrillation: a prospective, randomized, multi-centre, open label trial
- PMID: 36576323
- PMCID: PMC10062288
- DOI: 10.1093/europace/euac253
Ablation versus anti-arrhythmic therapy for reducing all hospital episodes from recurrent atrial fibrillation: a prospective, randomized, multi-centre, open label trial
Abstract
Aims: There is rising healthcare utilization related to the increasing incidence and prevalence of atrial fibrillation (AF) worldwide. Simplifying therapy and reducing hospital episodes would be a valuable development. The efficacy of a streamlined AF ablation approach was compared to drug therapy and a conventional catheter ablation technique for symptom control in paroxysmal AF.
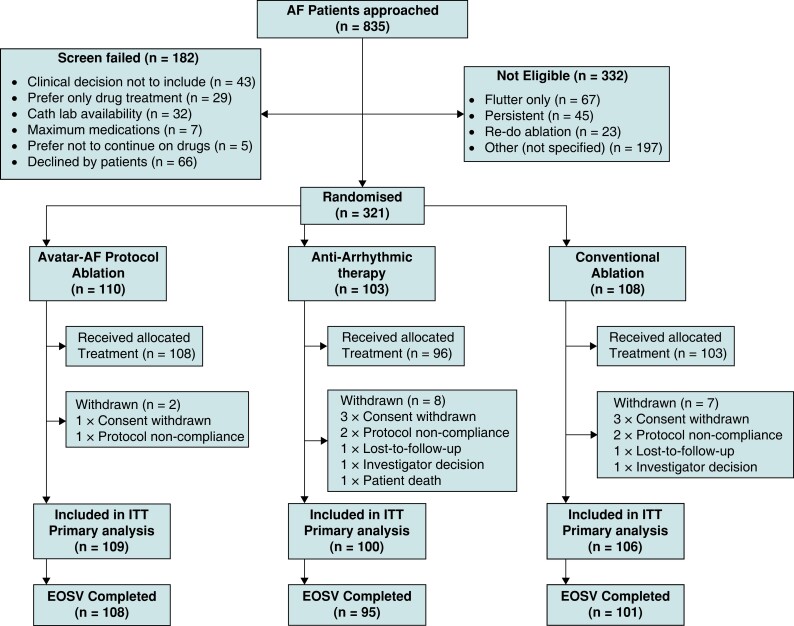
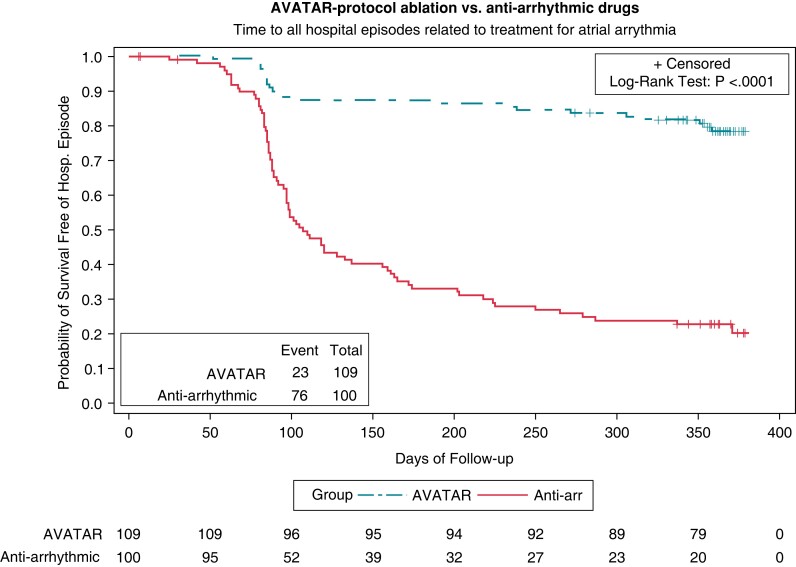
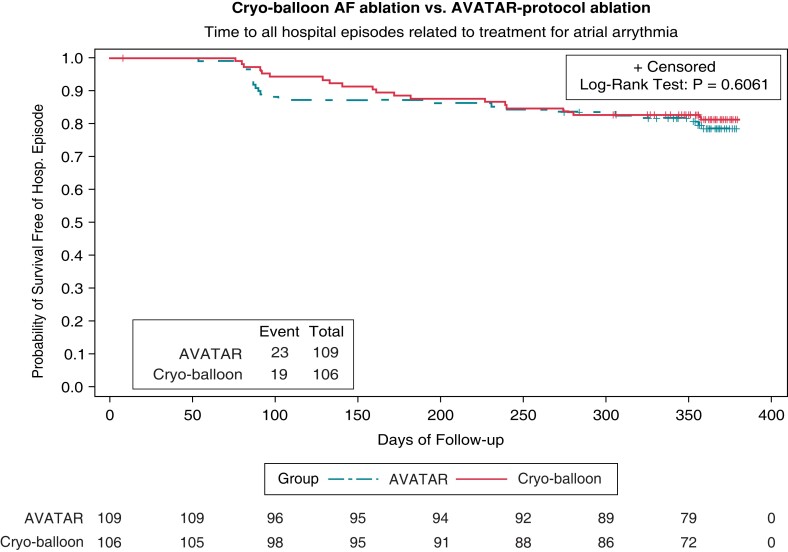
Methods and results: We recruited 321 patients with symptomatic paroxysmal AF to a prospective randomized, multi-centre, open label trial at 13 UK hospitals. Patients were randomized 1:1:1 to cryo-balloon ablation without electrical mapping with patients discharged same day [Ablation Versus Anti-arrhythmic Therapy for Reducing All Hospital Episodes from Recurrent (AVATAR) protocol]; optimization of drug therapy; or cryo-balloon ablation with confirmation of pulmonary vein isolation and overnight hospitalization. The primary endpoint was time to any hospital episode related to treatment for atrial arrhythmia. Secondary endpoints included complications of treatment and quality-of-life measures. The hazard ratio (HR) for a primary endpoint event occurring when comparing AVATAR protocol arm to drug therapy was 0.156 (95% CI, 0.097-0.250; P < 0.0001 by Cox regression). Twenty-three patients (21%) recorded an endpoint event in the AVATAR arm compared to 76 patients (74%) within the drug therapy arm. Comparing AVATAR and conventional ablation arms resulted in a non-significant HR of 1.173 (95% CI, 0.639-2.154; P = 0.61 by Cox regression) with 23 patients (21%) and 19 patients (18%), respectively, recording primary endpoint events (P = 0.61 by log-rank test).
Conclusion: The AVATAR protocol was superior to drug therapy for avoiding hospital episodes related to AF treatment, but conventional cryoablation was not superior to the AVATAR protocol. This could have wide-ranging implications on how demand for AF symptom control is met.
Trial registration: Clinical Trials Registration: NCT02459574.
Keywords: Ablation; Anti-arrhythmic; Atrial fibrillation; Cryoablation; Radiofrequency ablation.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: aside from the funding acknowledgements, no other support from any organization for the submitted work; P.K. has received consulting fees and research grants from Biosense-Webster, Abbott-Medical, Medtronic, and Boston-Scientific; J.M.C. has received a research grant and speaker fees from Medtronic; M.T. has received research grants from Medtronic, Biosense-Webster and Abbott Medical, and other support from Daiichi Sankyo and Abbott Medical; D.T. has received a travel grant for conference attendance from Medtronic UK, a consultancy fee from Abbott UK, and fees for teaching on a course from Medtronic UK Ltd, Boston Scientific Ltd, and Abbott UK; Z.W. has received speaker fees from Medtronic in relation to cardiac pacing; D.W.D. has received personal fees from Medtronic as a Consultant for the Medtronic AF division; I.M. and C.C. have received BHF Clinical Research Training Fellowship grants; P.K. and N.L. have a patent for Ripple Mapping which is licensed to Biosense-Webster with royalties paid to Imperial College. No other competing interests are declared.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist Cet al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J 2021;42:373–498. - PubMed
-
- Anderson JL, Gilbert EM, Alpert BL, Henthorn RW, Waldo AL, Bhandari AKet al. Prevention of symptomatic recurrences of paroxysmal atrial fibrillation in patients initially tolerating antiarrhythmic therapy. A multi-centre, double-blind, crossover study of flecainide and placebo with trans-telephonic monitoring. Flecainide supraventricular tachycardia study group. Circulation 1989;80:1557–70. - PubMed
-
- Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CLet al. Sotalol amiodarone atrial fibrillation efficacy trial (SAFE-T) investigators. Amiodarone versus sotalol for atrial fibrillation. N Engl J Med 2005;352:1861–72. - PubMed
-
- Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta Set al. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF study. J Am Coll Cardiol 2006;48:2340–7. - PubMed
-
- Stabile G, Bertaglia E, Senatore G, De Simone A, Zoppo F, Donnici Get al. Catheter ablation treatment in patients with drug-refractory atrial fibrillation: a prospective, multi-centre, randomized, controlled study (catheter ablation for the cure of atrial fibrillation study). Eur Heart J 2006;27:216–21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
