

Plague Meningitis: A Systematic Review of Clinical Course, Antimicrobial Treatment, and Outcomes
- PMID: 36576503
- PMCID: PMC10543819
- DOI: 10.1089/hs.2022.0081
Plague Meningitis: A Systematic Review of Clinical Course, Antimicrobial Treatment, and Outcomes
Abstract
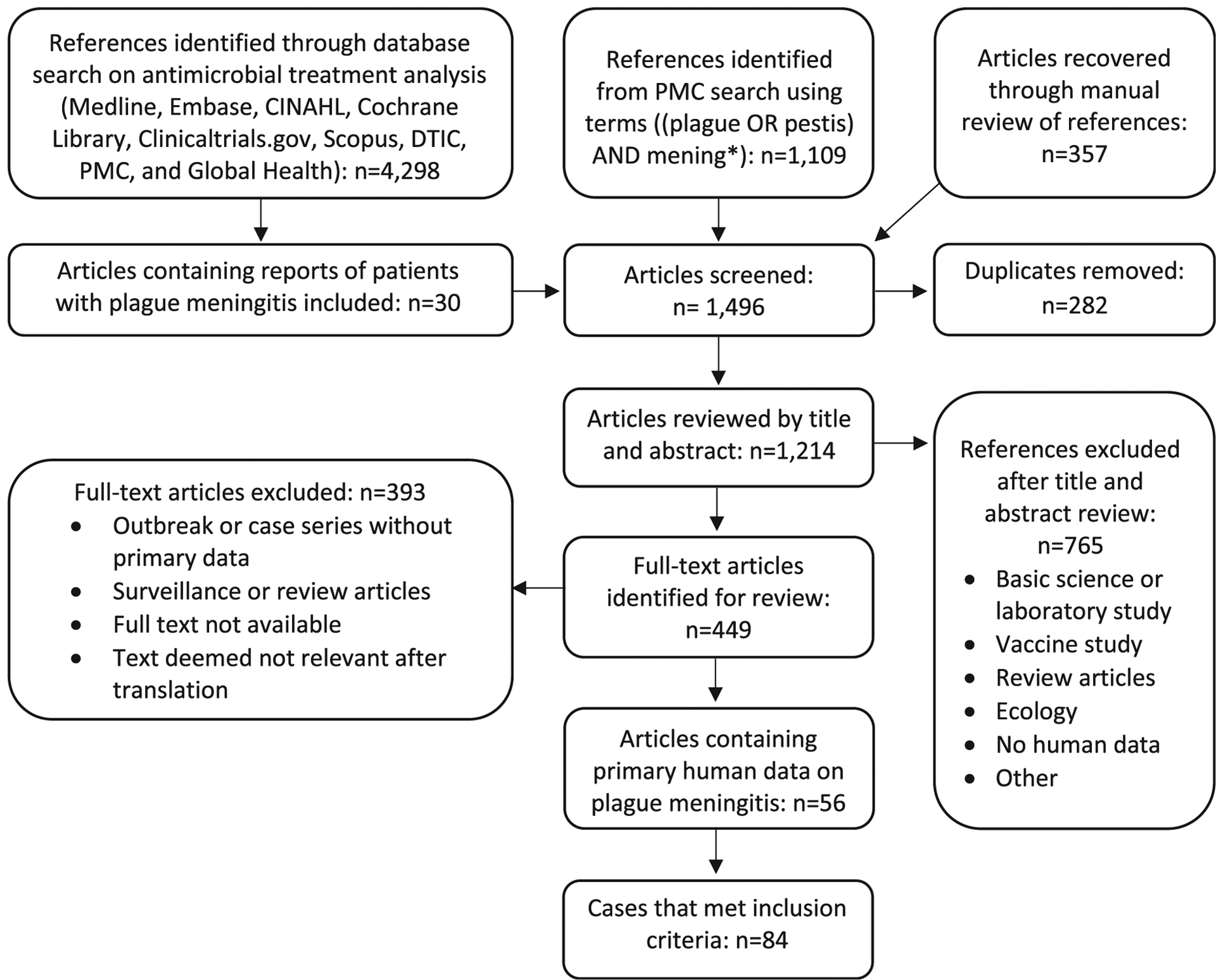
Plague meningitis is a serious and often fatal manifestation of Yersinia pestis infection. In the aftermath of a bioweapon attack with Y pestis, this typically rare manifestation may develop in a substantial number of patients, particularly if treatment delays occur. Risk factors, clinical evolution, and optimal treatment strategies for plague meningitis are not well understood. We searched PubMed Central and other databases for reports of plague meningitis in any language. Articles containing descriptions of patients with plague meningitis and their treatment and outcomes were included. Among 1,496 articles identified in our search, 56 articles describing 84 cases from 1898 to 2015 met inclusion criteria. The median age of patients was 16 years (range 6 weeks to 64 years); 68% were male. Most patients (n = 50, 60%) developed meningitis following primary bubonic plague. Common signs and symptoms included fever (n = 56, 66%), nuchal rigidity (n = 38, 45%), and headache (n = 33, 36%); 29% (n = 24) of patients had focal neurologic deficits such as cranial nerve abnormalities. Almost all (n = 23, 96%) of the 24 patients who did not receive antimicrobials died, and 42% (n = 25) of the 59 patients treated with antimicrobials died. The case fatality rate of patients grouped by antimicrobial received was 50% (1 out of 2) for fluoroquinolones, 19% (4 out of 21) for aminoglycosides, 14% (2 out of 14) for sulfonamides, 11% (2 out of 18) for chloramphenicol, and 0% (0 out of 13) for tetracyclines. Plague meningitis most often occurs as a complication of bubonic plague and can cause focal neurologic deficits. Survival is more likely in patients who receive antimicrobials; tetracyclines, aminoglycosides, and chloramphenicol had the lowest associated case fatality rates.
Keywords: Meningitis; Plague; Public health preparedness/response; Surveillance; Yersinia pestis.
Figures




References
-
- Cunha CB, Cunha BA. Impact of plague on human history. Infect Dis Clin North Am. 2006;20(2):253–272. - PubMed
-
- Bertherat E Plague around the world in 2019. Wkly Epidemiol Rec. 2019;94(25):289–292.
-
- Inglesby TV, Dennis DT, Henderson DA, et al. Plague as a biological weapon: medical and public health management. JAMA. 2000;283(17):2281–2290. - PubMed
-
- World Health Organization (WHO). Health Aspects of Chemical and Biological Weapons; Report of a WHO Group of Consultants. Geneva: WHO; 1970. https://apps.who.int/iris/handle/10665/39444
-
- Poland JD, Dennis DT. Diagnosis and clinical manifestations. In: Dennis DT, Gage KL, Gratz NG, Poland LD, Tikhomirov, eds. Plague Manual: Epidemiology, Distribution, Surveillance and Control. Geneva: World Health Organization; 1999:43–53. https://apps.who.int/iris/handle/10665/66010
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
