

Modeling Diagnostic Expertise in Cases of Irreducible Uncertainty: The Decision-Aligned Response Model
- PMID: 36576770
- PMCID: PMC9780042
- DOI: 10.1097/ACM.0000000000004918
Modeling Diagnostic Expertise in Cases of Irreducible Uncertainty: The Decision-Aligned Response Model
Abstract
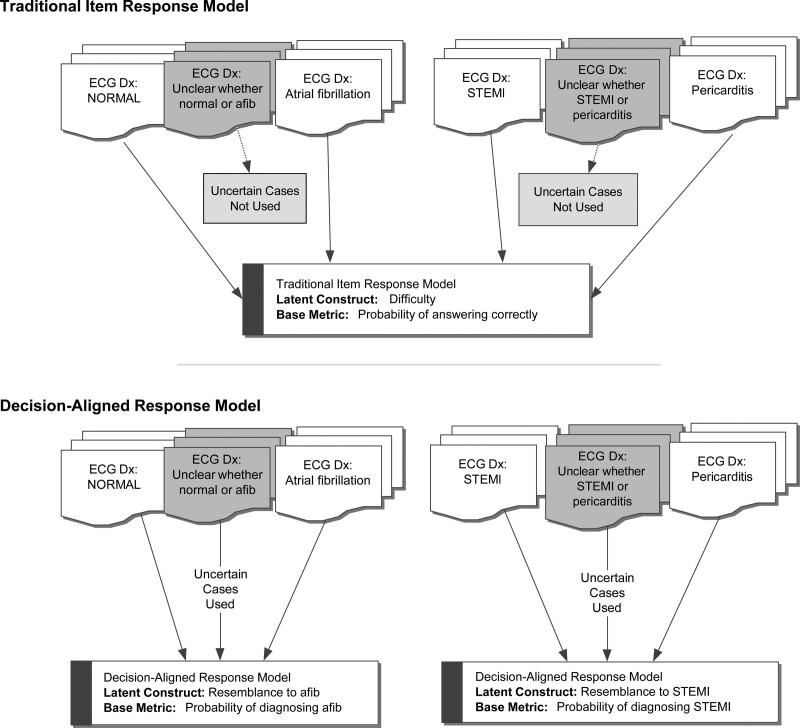
Purpose: Assessing expertise using psychometric models usually yields a measure of ability that is difficult to generalize to the complexity of diagnoses in clinical practice. However, using an item response modeling framework, it is possible to create a decision-aligned response model that captures a clinician's decision-making behavior on a continuous scale that fully represents competing diagnostic possibilities. In this proof-of-concept study, the authors demonstrate the necessary statistical conceptualization of this model using a specific electrocardiogram (ECG) example.
Method: The authors collected a range of ECGs with elevated ST segments due to either ST-elevation myocardial infarction (STEMI) or pericarditis. Based on pilot data, 20 ECGs were chosen to represent a continuum from "definitely STEMI" to "definitely pericarditis," including intermediate cases in which the diagnosis was intentionally unclear. Emergency medicine and cardiology physicians rated these ECGs on a 5-point scale ("definitely STEMI" to "definitely pericarditis"). The authors analyzed these ratings using a graded response model showing the degree to which each participant could separate the ECGs along the diagnostic continuum. The authors compared these metrics with the discharge diagnoses noted on chart review.
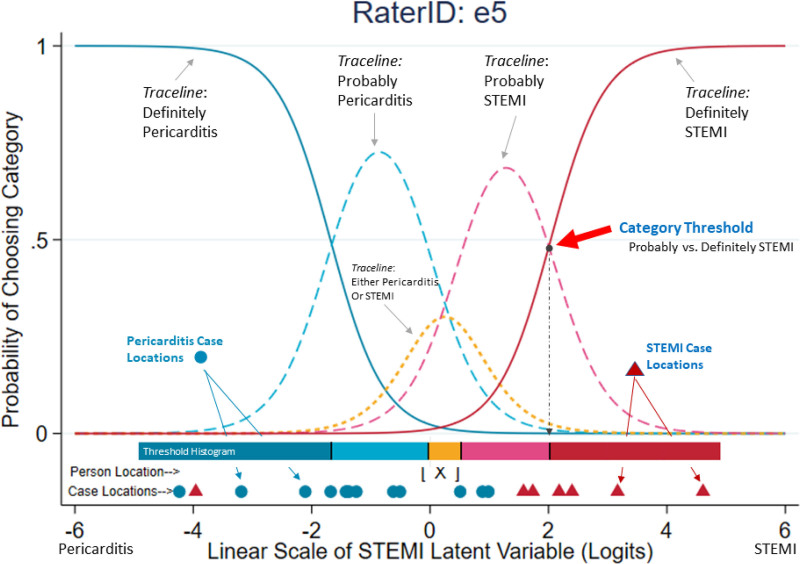
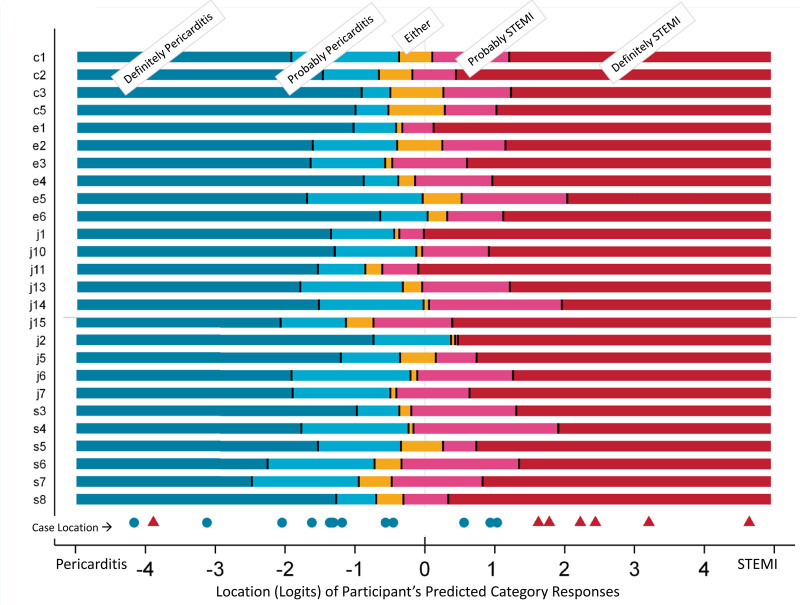
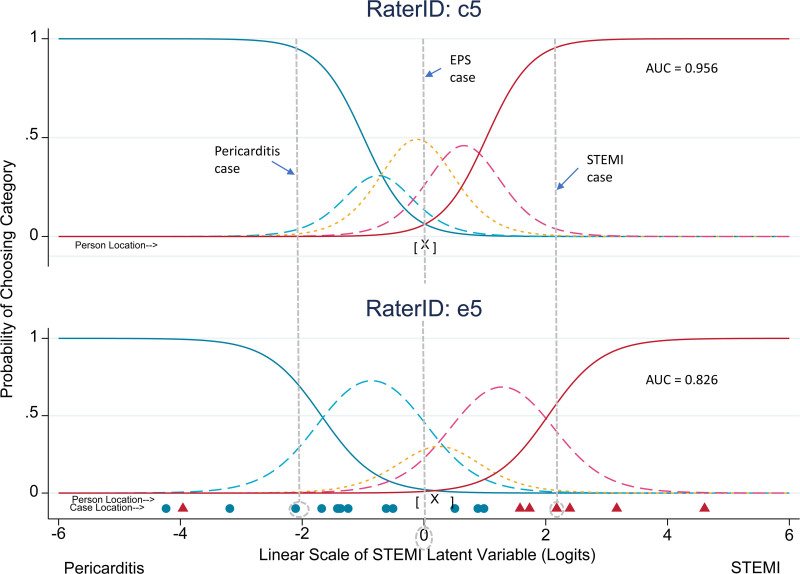
Results: Thirty-seven participants rated the ECGs. As desired, the ECGs represented a range of phenotypes, including cases where participants were uncertain in their diagnosis. The response model showed that participants varied both in their propensity to diagnose one condition over another and in where they placed the thresholds between the 5 diagnostic categories. The most capable participants were able to meaningfully use all categories, with precise thresholds between categories.
Conclusions: The authors present a decision-aligned response model that demonstrates the confusability of a particular ECG and the skill with which a clinician can distinguish 2 diagnoses along a continuum of confusability. These results have broad implications for testing and for learning to manage uncertainty in diagnosis.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Association of American Medical Colleges.
Conflict of interest statement
Figures
Similar articles
-
Estimating the Irreducible Uncertainty in Visual Diagnosis: Statistical Modeling of Skill Using Response Models.Med Decis Making. 2023 Aug;43(6):680-691. doi: 10.1177/0272989X231162095. Epub 2023 Jul 3. Med Decis Making. 2023. PMID: 37401184
-
Emergency physician accuracy in interpreting electrocardiograms with potential ST-segment elevation myocardial infarction: Is it enough?Acute Card Care. 2016 Mar;18(1):7-10. doi: 10.1080/17482941.2016.1234058. Epub 2016 Oct 19. Acute Card Care. 2016. PMID: 27759433
-
[Application of wearable 12-lead electrocardiogram devices in pre-hospital diagnosis of acute ST segment elevation myocardial infarction].Nan Fang Yi Ke Da Xue Xue Bao. 2022 Oct 20;42(10):1566-1571. doi: 10.12122/j.issn.1673-4254.2022.10.18. Nan Fang Yi Ke Da Xue Xue Bao. 2022. PMID: 36329593 Free PMC article. Chinese.
-
The Role of ECG in the Diagnosis and Risk Stratification of Acute Coronary Syndromes: an Old but Indispensable Tool.Curr Cardiol Rep. 2022 Feb;24(2):109-118. doi: 10.1007/s11886-021-01628-7. Epub 2022 Jan 13. Curr Cardiol Rep. 2022. PMID: 35028816 Review.
-
[STEMI mimics : ST elevations on ECG: alternative diagnoses to acute coronary occlusion].Med Klin Intensivmed Notfmed. 2023 Feb;118(1):35-44. doi: 10.1007/s00063-021-00882-5. Epub 2021 Oct 28. Med Klin Intensivmed Notfmed. 2023. PMID: 34709428 Free PMC article. Review. German.
References
-
- Tamblyn R, Abrahamowicz M, Dauphinee WD, et al. . Association between licensure examination scores and practice in primary care. JAMA. 2002;288:3019–3026. - PubMed
-
- Ilgen JS, Eva KW, de Bruin A, Cook DA, Regehr G. Comfort with uncertainty: Reframing our conceptions of how clinicians navigate complex clinical situations. Adv Health Sci Educ Theory Pract. 2019;24:797–809. - PubMed
-
- Zhang S, Petersen JH. Quantifying rater variation for ordinal data using a rating scale model. Stat Med. 2018;37:2223–2237. - PubMed
-
- Schwarz RD. Trace lines for classification decisions. Appl Meas Edu. 1998;4:311–330.
-
- Baldwin P, Bernstein J, Wainer H. Hip psychometrics. Stat Med. 2009;28:2277–2292. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
