

Performance of Cardiovascular Risk Prediction Models Among People Living With HIV: A Systematic Review and Meta-analysis
- PMID: 36576812
- PMCID: PMC9857084
- DOI: 10.1001/jamacardio.2022.4873
Performance of Cardiovascular Risk Prediction Models Among People Living With HIV: A Systematic Review and Meta-analysis
Abstract
Importance: Extant data on the performance of cardiovascular disease (CVD) risk score models in people living with HIV have not been synthesized.
Objective: To synthesize available data on the performance of the various CVD risk scores in people living with HIV.
Data sources: PubMed and Embase were searched from inception through January 31, 2021.
Study selection: Selected studies (1) were chosen based on cohort design, (2) included adults with a diagnosis of HIV, (3) assessed CVD outcomes, and (4) had available data on a minimum of 1 CVD risk score.
Data extraction and synthesis: Relevant data related to study characteristics, CVD outcome, and risk prediction models were extracted in duplicate. Measures of calibration and discrimination are presented in tables and qualitatively summarized. Additionally, where possible, estimates of discrimination and calibration measures were combined and stratified by type of risk model.
Main outcomes and measures: Measures of calibration and discrimination.
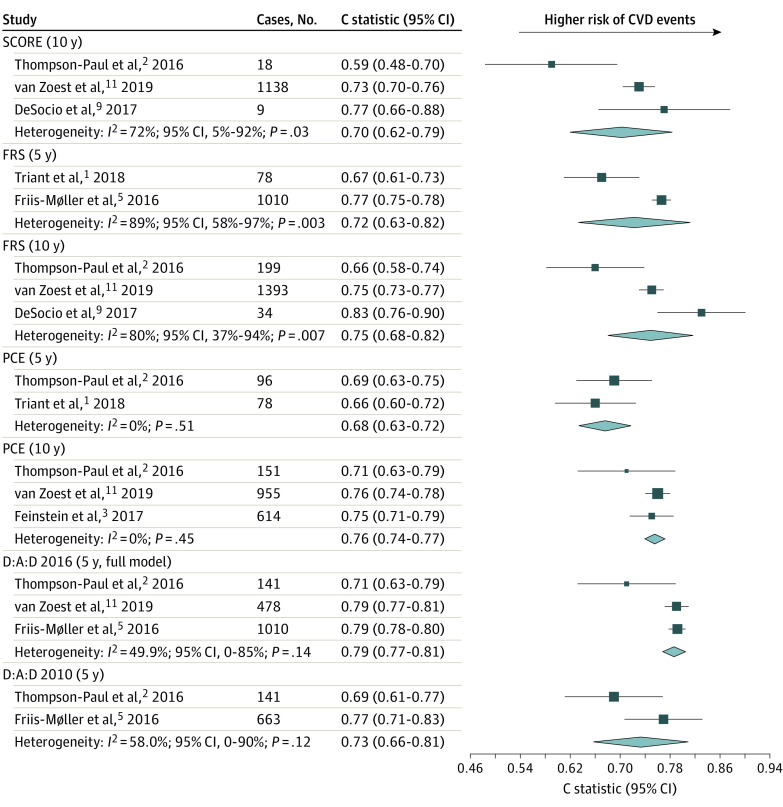
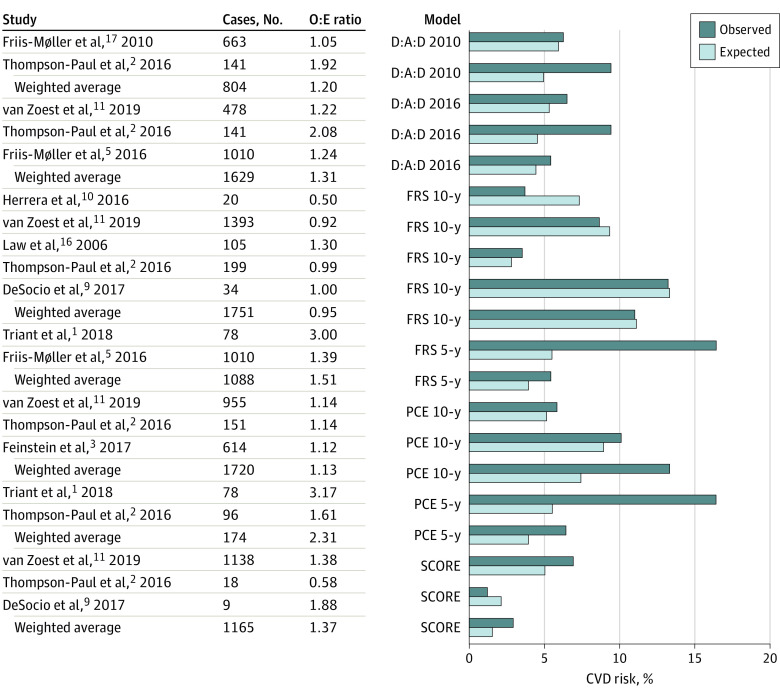
Results: Nine unique observational studies involving 75 304 people (weighted average age, 42 years; 59 490 male individuals [79%]) living with HIV were included. In the studies reporting these data, 86% were receiving antiretroviral therapy and had a weighted average CD4+ count of 449 cells/μL. Included in the study were current smokers (50%), patients with diabetes (5%), and patients with hypertension (25%). Ten risk prediction scores (6 in the general population and 4 in the HIV-specific population) were analyzed. Most risk scores had a moderate performance in discrimination (C statistic: 0.7-0.8), without a significant difference in performance between the risk scores of the general and HIV-specific populations. One of the HIV-specific risk models (Data Collection on Adverse Effects of Anti-HIV Drugs Cohort 2016) and 2 of the general population risk models (Framingham Risk Score [FRS] and Pooled Cohort Equation [PCE] 10 year) had the highest performance in discrimination. In general, models tended to underpredict CVD risk, except for FRS and PCE 10-year scores, which were better calibrated. There was substantial heterogeneity across the studies, with only a few studies contributing data for each risk score.
Conclusions and relevance: Results of this systematic review and meta-analysis suggest that general population and HIV-specific CVD risk models had comparable, moderate discrimination ability in people living with HIV, with a general tendency to underpredict risk. These results reinforce the current recommendations provided by the American College of Cardiology/American Heart Association guidelines to consider HIV as a risk-enhancing factor when estimating CVD risk.
Conflict of interest statement
Figures
Comment in
-
Science and ART-Cardiovascular Disease Risk Assessment in HIV.JAMA Cardiol. 2023 Feb 1;8(2):107-108. doi: 10.1001/jamacardio.2022.4880. JAMA Cardiol. 2023. PMID: 36576806 No abstract available.
Similar articles
-
Predictive Performance of Cardiovascular Disease Risk Prediction Algorithms in People Living With HIV.J Acquir Immune Defic Syndr. 2019 Aug 15;81(5):562-571. doi: 10.1097/QAI.0000000000002069. J Acquir Immune Defic Syndr. 2019. PMID: 31045648
-
Cardiovascular Disease Risk Prediction in the HIV Outpatient Study.Clin Infect Dis. 2016 Dec 1;63(11):1508-1516. doi: 10.1093/cid/ciw615. Epub 2016 Sep 9. Clin Infect Dis. 2016. PMID: 27613562 Free PMC article.
-
Cardiovascular Risk Estimation Is Suboptimal in People With HIV.J Am Heart Assoc. 2024 May 21;13(10):e029228. doi: 10.1161/JAHA.123.029228. Epub 2024 May 18. J Am Heart Assoc. 2024. PMID: 38761071 Free PMC article.
-
Prediction models for cardiovascular disease risk among people living with HIV: A systematic review and meta-analysis.Front Cardiovasc Med. 2023 Mar 23;10:1138234. doi: 10.3389/fcvm.2023.1138234. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37034346 Free PMC article. Review.
-
Performance of the Framingham risk models and pooled cohort equations for predicting 10-year risk of cardiovascular disease: a systematic review and meta-analysis.BMC Med. 2019 Jun 13;17(1):109. doi: 10.1186/s12916-019-1340-7. BMC Med. 2019. PMID: 31189462 Free PMC article.
Cited by
-
Polygenic Scores and Preclinical Cardiovascular Disease in Individuals With HIV: Insights From the REPRIEVE Trial.J Am Heart Assoc. 2024 Apr 2;13(7):e033413. doi: 10.1161/JAHA.123.033413. Epub 2024 Mar 27. J Am Heart Assoc. 2024. PMID: 38533953 Free PMC article.
-
Association between the triglyceride to high-density lipoprotein cholesterol ratio and cardiovascular diseases in people living with human immunodeficiency virus: Evidence from a retrospectively cohort study 2005-2022.Chin Med J (Engl). 2024 Nov 20;137(22):2712-2719. doi: 10.1097/CM9.0000000000003326. Epub 2024 Oct 25. Chin Med J (Engl). 2024. PMID: 39450977 Free PMC article.
-
Association of prior tuberculosis with altered cardiometabolic profiles of people with HIV: A comparative cross-sectional study in Uganda.medRxiv [Preprint]. 2025 Mar 20:2025.03.19.25324234. doi: 10.1101/2025.03.19.25324234. medRxiv. 2025. Update in: J Clin Tuberc Other Mycobact Dis. 2025 Apr 01;39:100523. doi: 10.1016/j.jctube.2025.100523. PMID: 40166552 Free PMC article. Updated. Preprint.
-
Prediction of Cardiovascular Risk Among People with HIV Using the PREVENT Equations Compared to the Pooled Cohort Equations.J Gen Intern Med. 2025 Jun 6. doi: 10.1007/s11606-025-09642-z. Online ahead of print. J Gen Intern Med. 2025. PMID: 40481382
-
Recommendations for prediction models in clinical practice guidelines for cardiovascular diseases are over-optimistic: a global survey utilizing a systematic literature search.Front Cardiovasc Med. 2024 Oct 17;11:1449058. doi: 10.3389/fcvm.2024.1449058. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39484015 Free PMC article.
References
-
- Friis-Møller N, Ryom L, Smith C, et al. ; D:A:D study group . An updated prediction model of the global risk of cardiovascular disease in HIV-positive persons: the Data-CSollection on Adverse Effects of Anti-HIV Drugs (D:A:D) study. Eur J Prev Cardiol. 2016;23(2):214-223. doi:10.1177/2047487315579291 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
