

Cost-effectiveness of Laparoscopic vs Open Gastrectomy for Gastric Cancer: An Economic Evaluation Alongside a Randomized Clinical Trial
- PMID: 36576822
- PMCID: PMC9856973
- DOI: 10.1001/jamasurg.2022.6337
Cost-effectiveness of Laparoscopic vs Open Gastrectomy for Gastric Cancer: An Economic Evaluation Alongside a Randomized Clinical Trial
Abstract
Importance: Laparoscopic gastrectomy is rapidly being adopted worldwide as an alternative to open gastrectomy to treat gastric cancer. However, laparoscopic gastrectomy might be more expensive as a result of longer operating times and more expensive surgical materials. To date, the cost-effectiveness of both procedures has not been prospectively evaluated in a randomized clinical trial.
Objective: To evaluate the cost-effectiveness of laparoscopic compared with open gastrectomy.
Design, setting, and participants: In this multicenter randomized clinical trial of patients undergoing total or distal gastrectomy in 10 Dutch tertiary referral centers, cost-effectiveness data were collected alongside a multicenter randomized clinical trial on laparoscopic vs open gastrectomy for resectable gastric adenocarcinoma (cT1-4aN0-3bM0). A modified societal perspective and 1-year time horizon were used. Costs were calculated on the individual patient level by using hospital registry data and medical consumption and productivity loss questionnaires. The unit costs of laparoscopic and open gastrectomy were calculated bottom-up. Quality-adjusted life-years (QALYs) were calculated with the EuroQol 5-dimension questionnaire, in which a value of 0 indicates death and 1 indicates perfect health. Missing questionnaire data were imputed with multiple imputation. Bootstrapping was performed to estimate the uncertainty surrounding the cost-effectiveness. The study was conducted from March 17, 2015, to August 20, 2018. Data analyses were performed between September 1, 2020, and November 17, 2021.
Interventions: Laparoscopic vs open gastrectomy.
Main outcomes and measures: Evaluations in this cost-effectiveness analysis included total costs and QALYs.
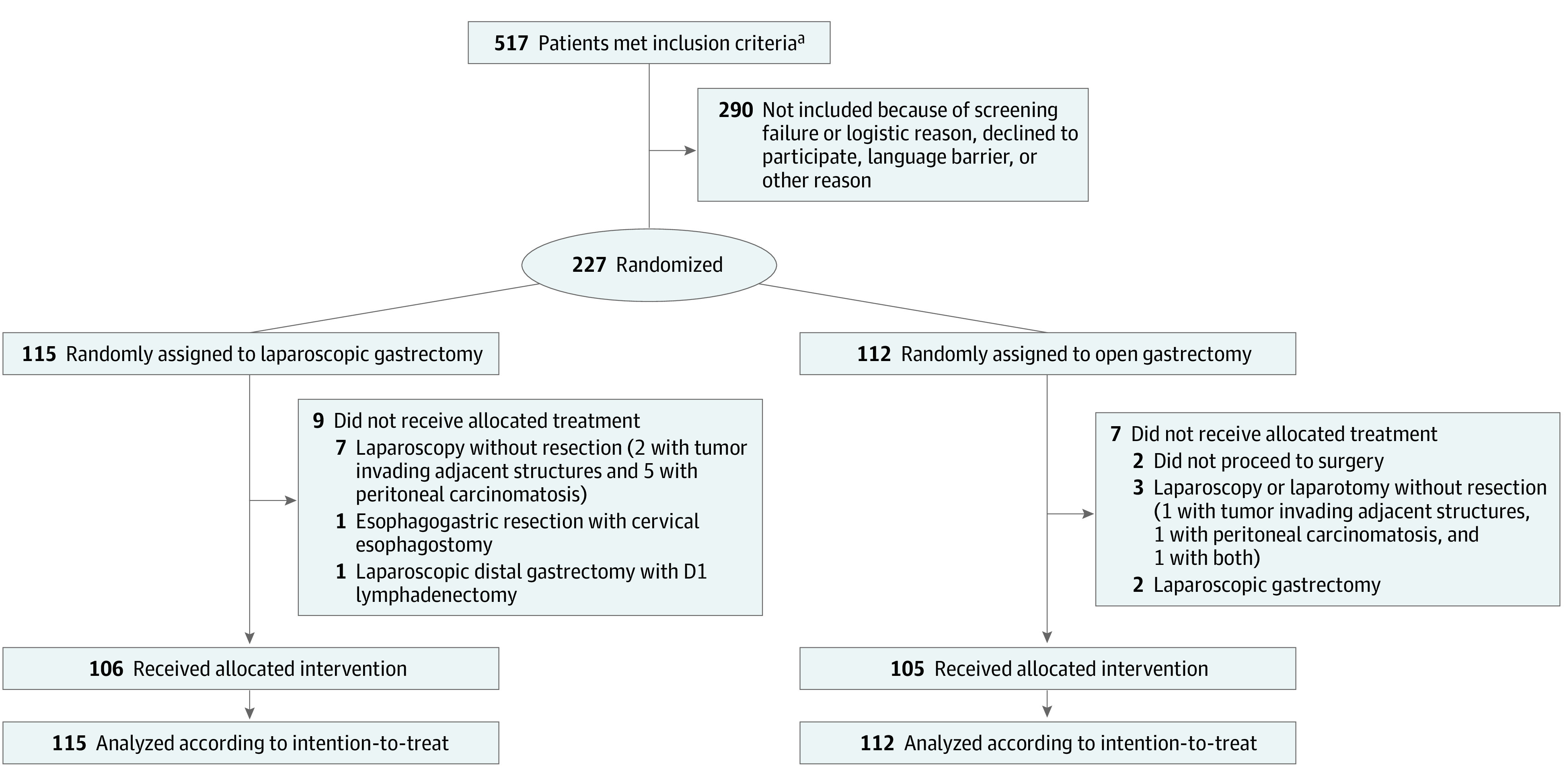
Results: Between 2015 and 2018, 227 patients were included. Mean (SD) age was 67.5 (11.7) years, and 140 were male (61.7%). Unit costs for initial surgery were calculated to be €8124 (US $8087) for laparoscopic total gastrectomy, €7353 (US $7320) for laparoscopic distal gastrectomy, €6584 (US $6554) for open total gastrectomy, and €5893 (US $5866) for open distal gastrectomy. Mean total costs after 1-year follow-up were €26 084 (US $25 965) in the laparoscopic group and €25 332 (US $25 216) in the open group (difference, €752 [US $749; 3.0%]). Mean (SD) QALY contributions during 1 year were 0.665 (0.298) in the laparoscopic group and 0.686 (0.288) in the open group (difference, -0.021). Bootstrapping showed that these differences between treatment groups were relatively small compared with the uncertainty of the analysis.
Conclusions and relevance: Although the laparoscopic gastrectomy itself was more expensive, after 1-year follow-up, results suggest that differences in both total costs and effectiveness were limited between laparoscopic and open gastrectomy. These results support centers' choosing, based on their own preference, whether to (de)implement laparoscopic gastrectomy as an alternative to open gastrectomy.
Conflict of interest statement
Figures


Comment in
-
Assessing Cost-effectiveness From the LOGICA Trial-Is Laparoscopic Gastrectomy Worth the Cost?JAMA Surg. 2023 Feb 1;158(2):129. doi: 10.1001/jamasurg.2022.6353. JAMA Surg. 2023. PMID: 36576818 Free PMC article. No abstract available.
References
-
- Al-Batran SE, Homann N, Pauligk C, et al. ; FLOT4-AIO Investigators . Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957. doi:10.1016/S0140-6736(18)32557-1 - DOI - PubMed
-
- Brenkman HJF, Ruurda JP, Verhoeven RHA, van Hillegersberg R. Safety and feasibility of minimally invasive gastrectomy during the early introduction in the Netherlands: short-term oncological outcomes comparable to open gastrectomy. Gastric Cancer. 2017;20(5):853-860. doi:10.1007/s10120-017-0695-8 - DOI - PMC - PubMed
-
- Dutch Upper GI Cancer Audit (DUCA) annual report 2019. Article in Dutch. DICA. Accessed August 24, 2021. https://dica.nl/jaarrapportage-2019/duca
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
