

IGF1 deficiency integrates stunted growth and neurodegeneration in Down syndrome
- PMID: 36577365
- PMCID: PMC9876612
- DOI: 10.1016/j.celrep.2022.111883
IGF1 deficiency integrates stunted growth and neurodegeneration in Down syndrome
Abstract
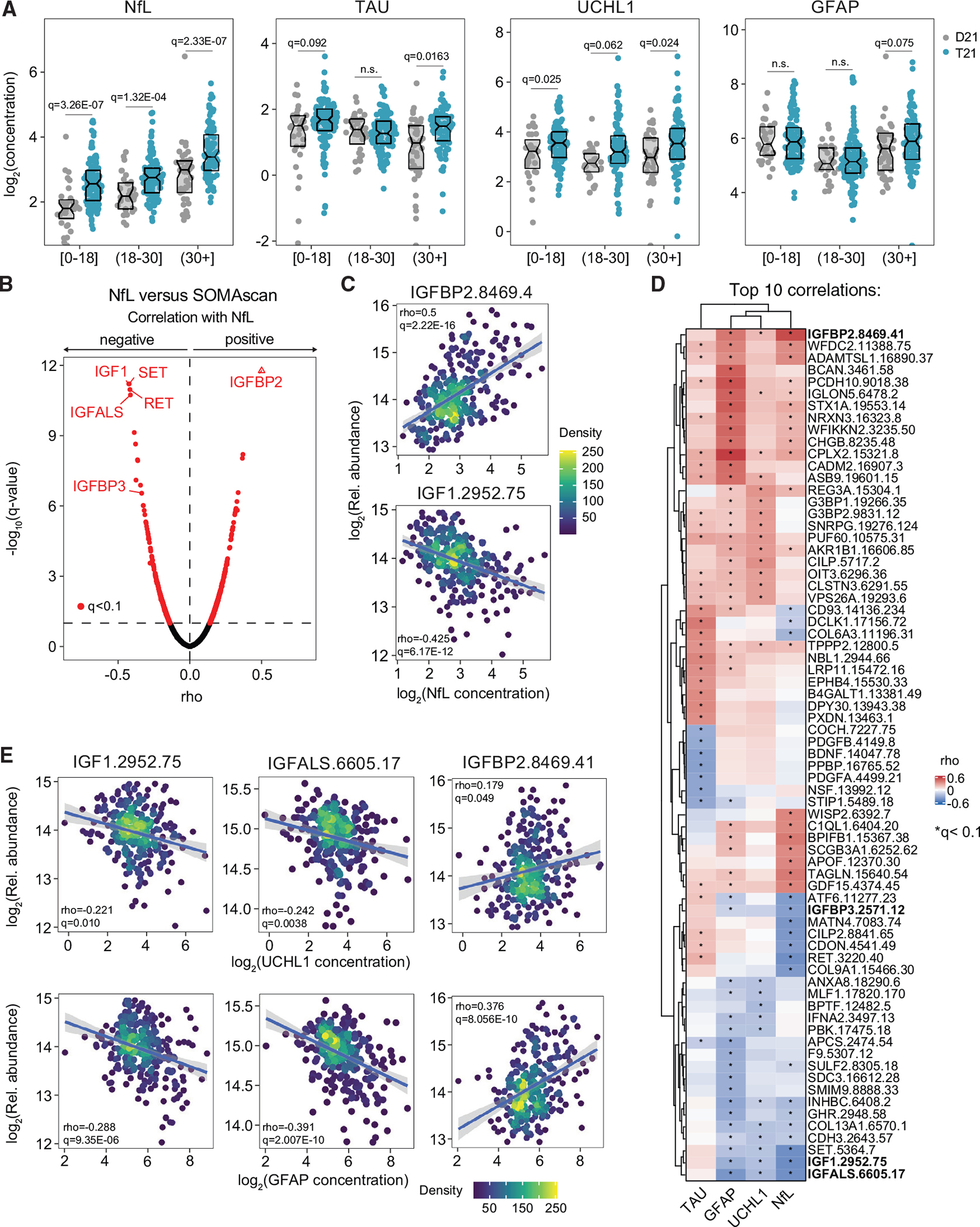
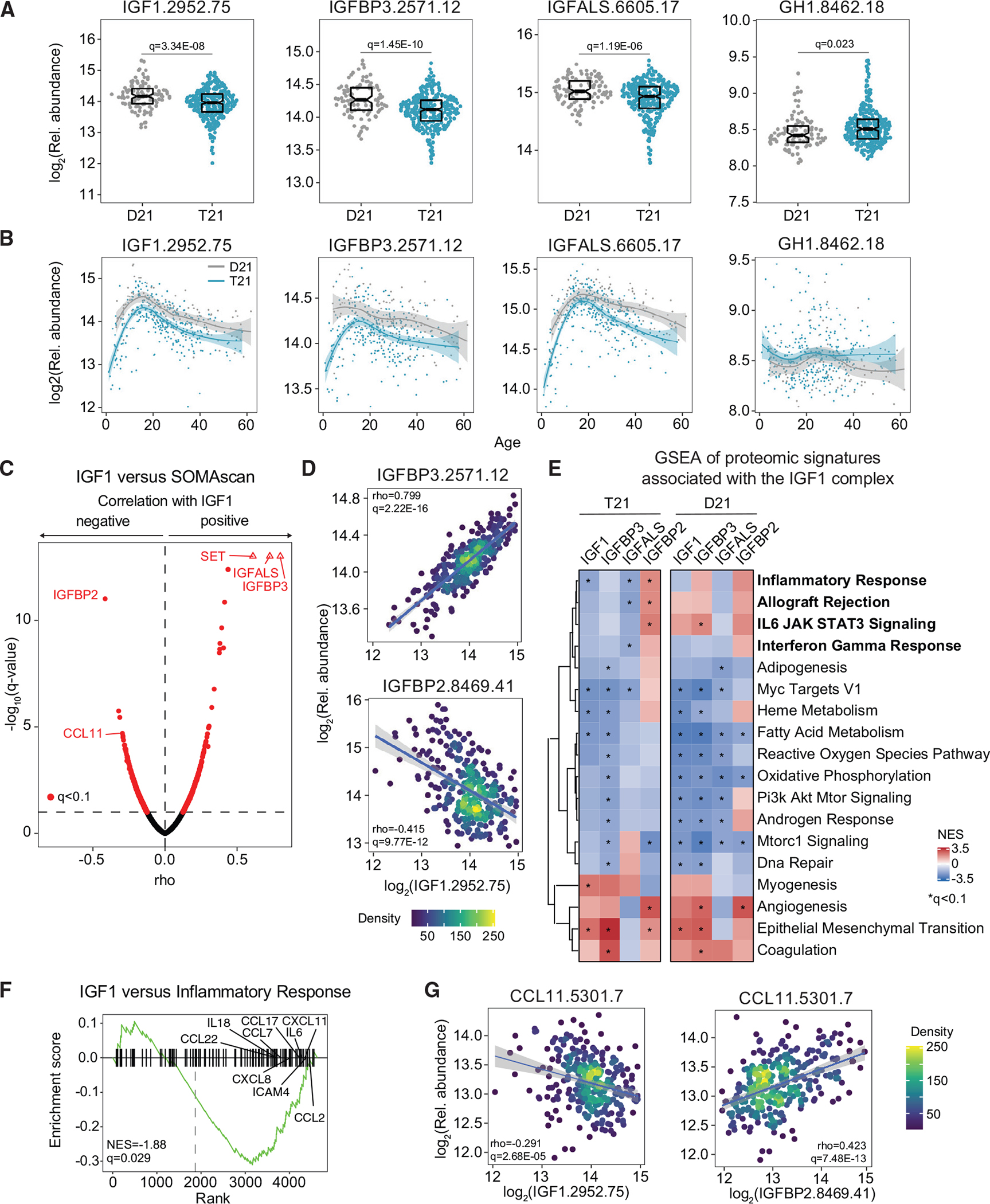
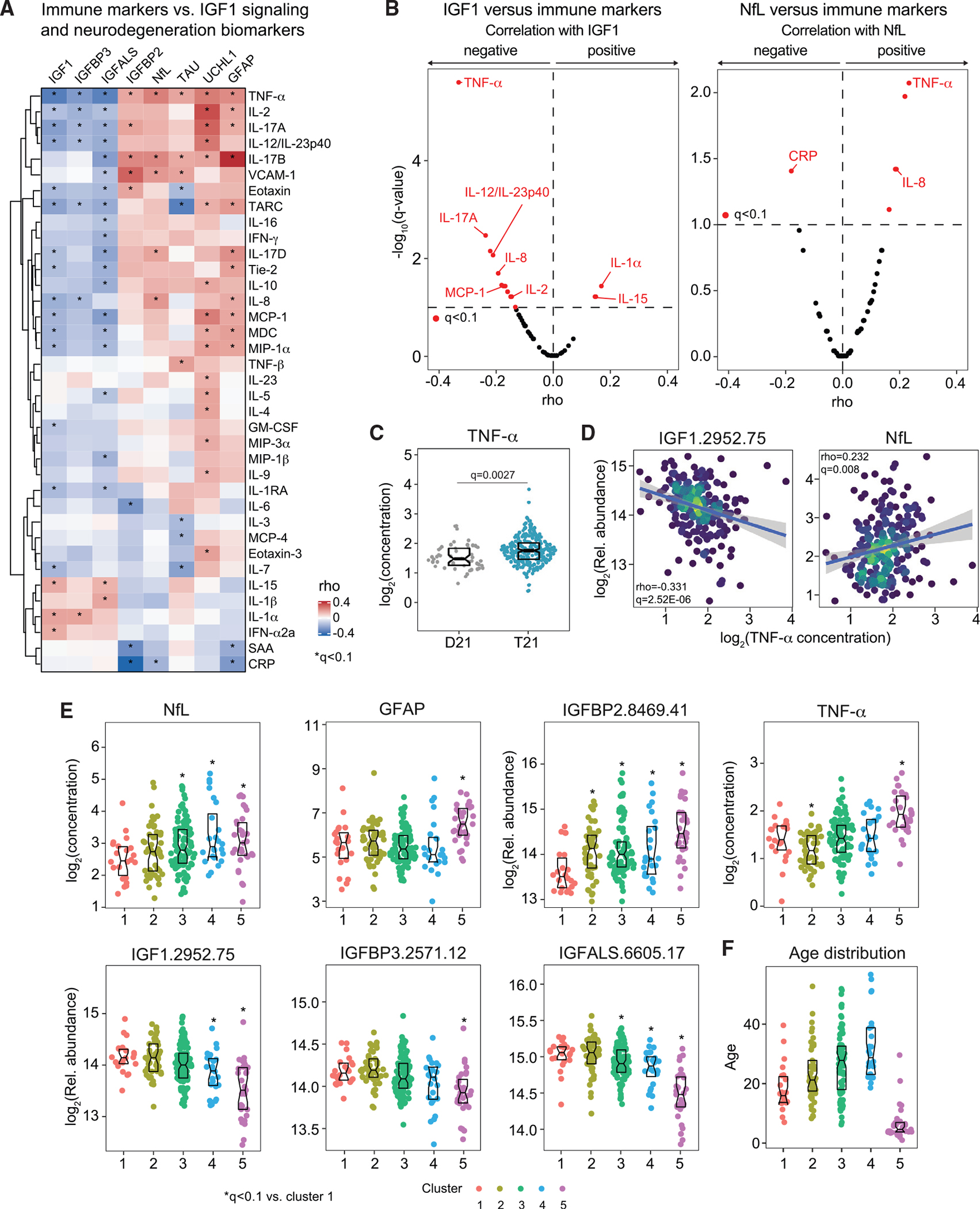
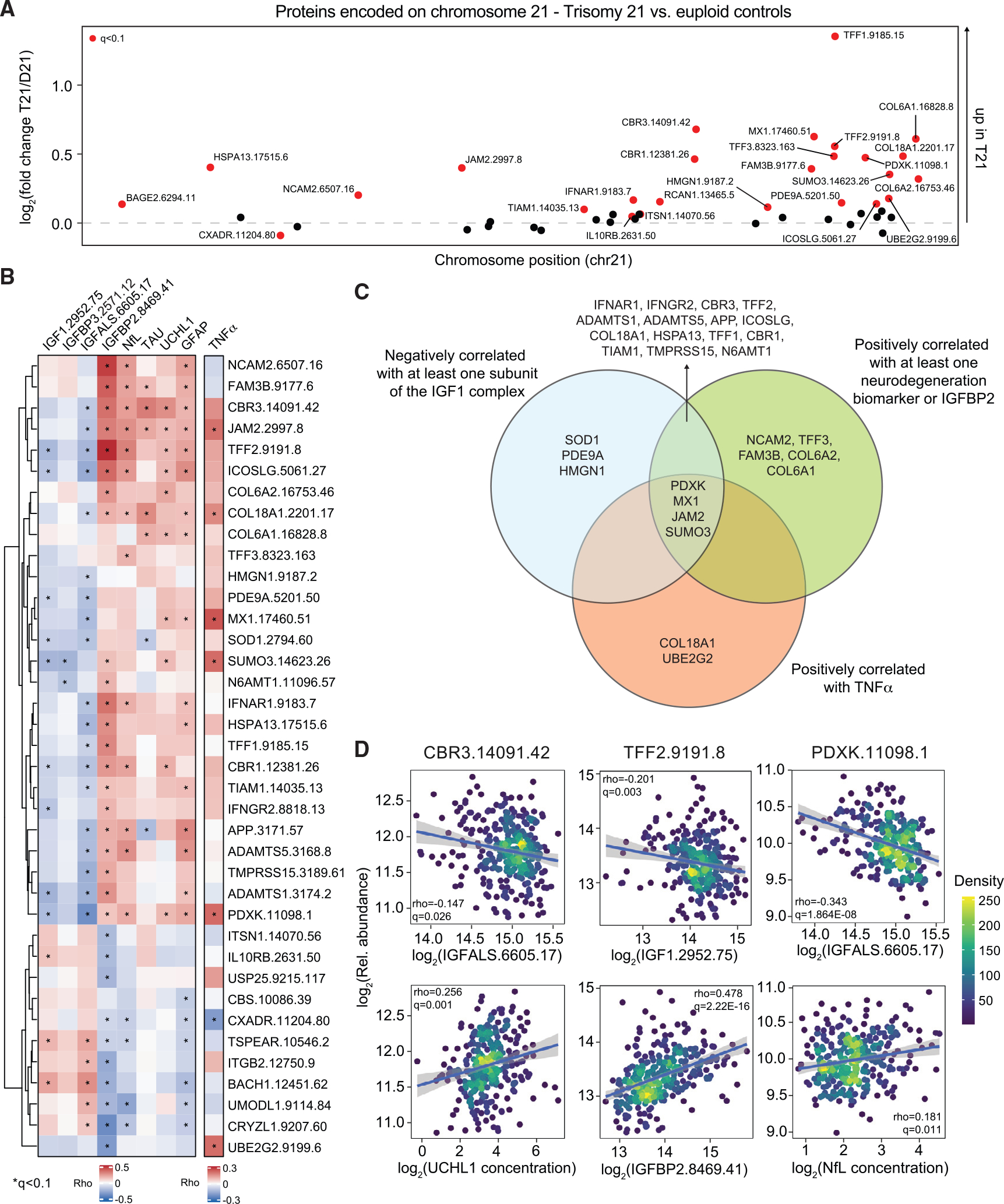
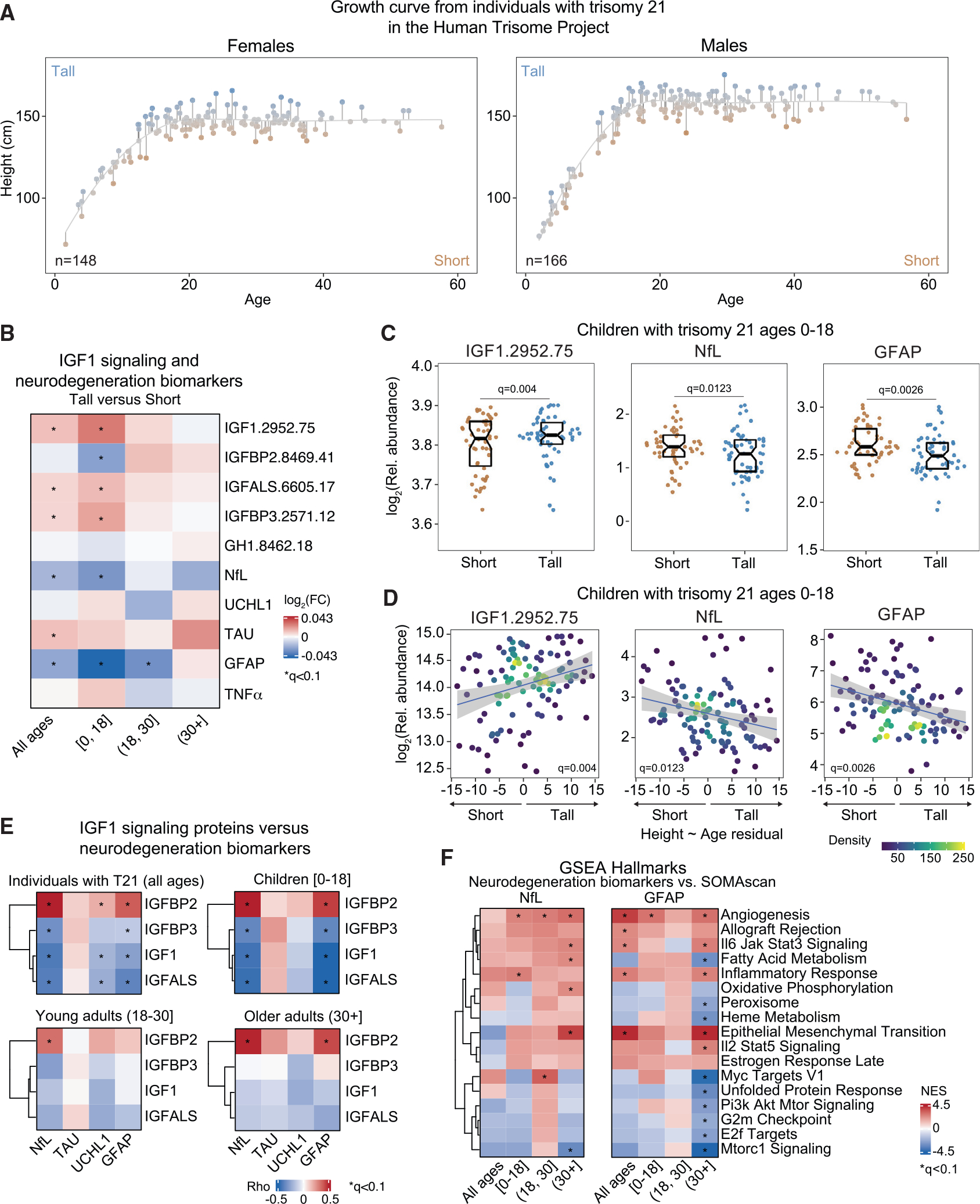
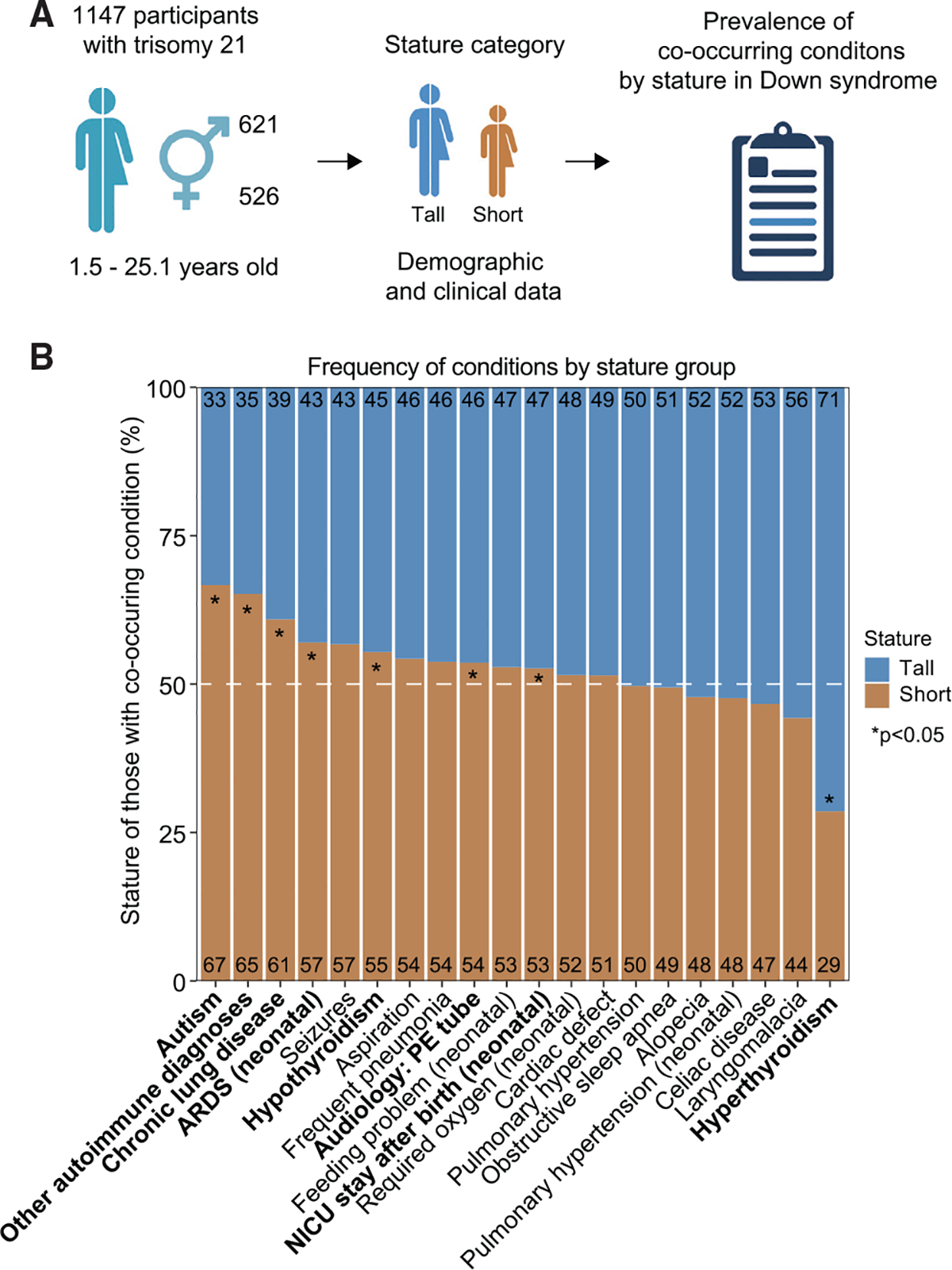
Down syndrome (DS), the genetic condition caused by trisomy 21 (T21), is characterized by stunted growth, cognitive impairment, and increased risk of diverse neurological conditions. Although signs of lifelong neurodegeneration are well documented in DS, the mechanisms underlying this phenotype await elucidation. Here we report a multi-omics analysis of neurodegeneration and neuroinflammation biomarkers, plasma proteomics, and immune profiling in a diverse cohort of more than 400 research participants. We identified depletion of insulin growth factor 1 (IGF1), a master regulator of growth and brain development, as the top biosignature associated with neurodegeneration in DS. Individuals with T21 display chronic IGF1 deficiency downstream of growth hormone production, associated with a specific inflammatory profile involving elevated tumor necrosis factor alpha (TNF-α). Shorter children with DS show stronger IGF1 deficiency, elevated biomarkers of neurodegeneration, and increased prevalence of autism and other conditions. These results point to disruption of IGF1 signaling as a potential contributor to stunted growth and neurodegeneration in DS.
Keywords: Alzheimer’s disease; CP: Developmental biology; CP: Neuroscience; autism; growth hormone; inflammation; insulin growth factor; mecasermin; neuroinflammation.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests J.M.E. has provided consulting services for Elli Lily and Co. and Gilead Sciences Inc. and serves on the advisory board of Perha Pharmaceuticals and on the editorial board of Cell Reports.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
