

Haploidentical Versus Matched Unrelated Donor Transplants Using Post-Transplantation Cyclophosphamide for Lymphomas
- PMID: 36577482
- PMCID: PMC10316698
- DOI: 10.1016/j.jtct.2022.11.028
Haploidentical Versus Matched Unrelated Donor Transplants Using Post-Transplantation Cyclophosphamide for Lymphomas
Abstract
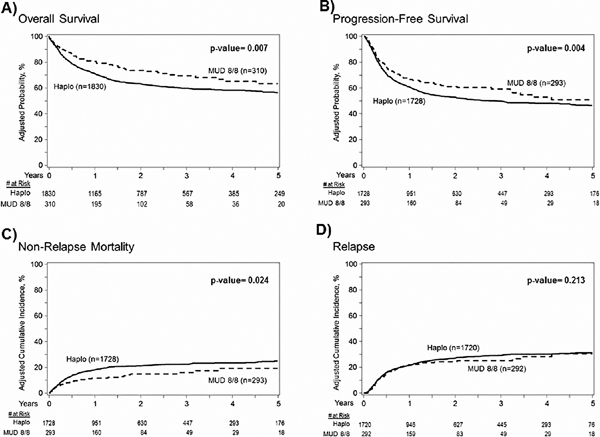
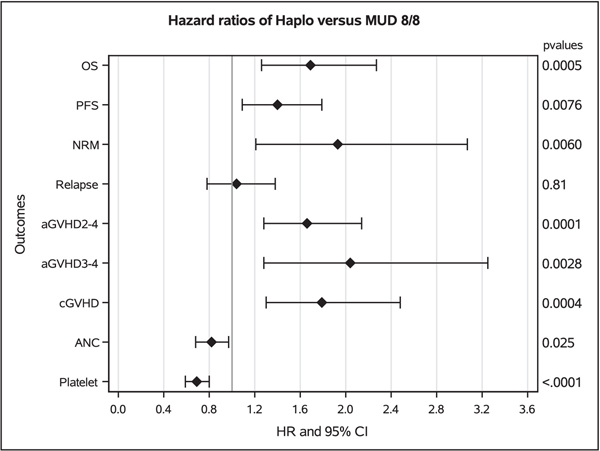
When using post-transplantation cyclophosphamide (PTCy) graft-versus-host disease (GVHD) prophylaxis for lymphoma patients, it is currently unknown whether a matched unrelated donor (MUD) or a haploidentical related donor is preferable if both are available. In this study we wanted to test whether using a haploidentical donor has the same results of a MUD. A total of 2140 adults (34% Center for International Blood and Marrow Transplant Research, 66% European Society for Blood and Marrow Transplantation registry) aged ≥18 years who received their first haploidentical hematopoietic cell transplantation (haplo-HCT) or MUD-HCT (8/8 match at HLA-loci A, B, C, and DRB1) for lymphoma using PTCy-based GVHD prophylaxis from 2010 to 2019 were retrospectively analyzed. The majority of both MUD and haploidentical HCTs received reduced intensity/nonmyeloablative conditioning (74% and 77%, respectively) and used a peripheral blood stem cell graft (91% and 60%, respectively) and a 3-drug GVHD prophylaxis (PTCy + calcineurin inhibitor + MMF in 54% and 90%, respectively). Haploidentical HCT has less favorable results versus MUD cohort in terms of overall mortality (hazard ratio [HR= = 1.69; 95% confidence interval [CI], 1.30-2.27; P < .001), progression-free survival (HR=1.39; 95% CI, 1.10-1.79; P = .008), nonrelapse mortality (HR = 1.93; 95% CI, 1.21-3.07; P = .006), platelet engraftment (HR = 0.69; 95% CI, 0.59-0.80; P < .001), acute grade 2-4 GVHD incidence (HR = 1.65; 95% CI, 1.28-2.14; P < .001), and chronic GVHD (HR = 1.79; 95% CI, 1.30-2.48, P < .001). No significant differences were observed in terms of relapse and neutrophil engraftment. Adjusting for propensity score yielded similar results. Whenever MUD is available in a timely manner, it should be preferred over a haploidentical donor when using PTCy-based GVHD prophylaxis for patients with lymphoma.
Keywords: Haploidentical donor; Lymphoma; Matched unrelated donor; Post-transplant cyclophosphamide.
Copyright © 2022 The American Society for Transplantation and Cellular Therapy. All rights reserved.
Conflict of interest statement
Declaration of interests
We declare no other competing interests for the execution of this study
Figures
References
-
- on behalf of the Japan Study Group for Cell Therapy and Transplantation (JSCT), Sugita J, Kagaya Y, et al. Myeloablative and reduced-intensity conditioning in HLA-haploidentical peripheral blood stem cell transplantation using post-transplant cyclophosphamide. Bone Marrow Transplant 2019; 54: 432–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
