

Intraductal oncocytic papillary neoplasm arising in Peutz-Jeghers Syndrome bile duct: a unique case report
- PMID: 36578081
- PMCID: PMC9795596
- DOI: 10.1186/s13000-022-01275-8
Intraductal oncocytic papillary neoplasm arising in Peutz-Jeghers Syndrome bile duct: a unique case report
Abstract
Background: Peutz-Jeghers syndrome (PJS) is a rare, autosomal dominant disorder caused by germline mutations of STK11/LKB1, with an increased risk of tumors at multiple sites. Intraductal oncocytic papillary neoplasm (IOPN) is a unique subtype of intraductal papillary neoplasm of the bile duct (IPNB) defined by a premalignant neoplasm with intraductal papillary or villous growth of biliary-type epithelium. IOPN has a distinct mutation profile compared with both IPNB and intraductal papillary mucinous neoplasm (IPMN).
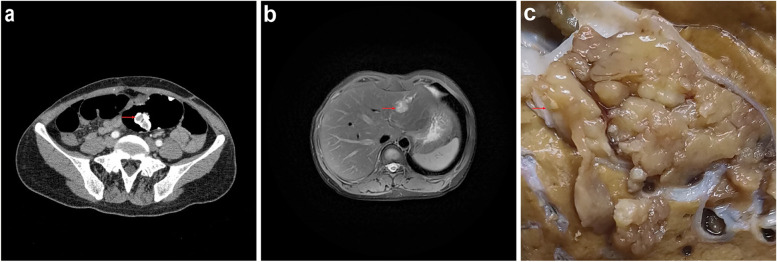
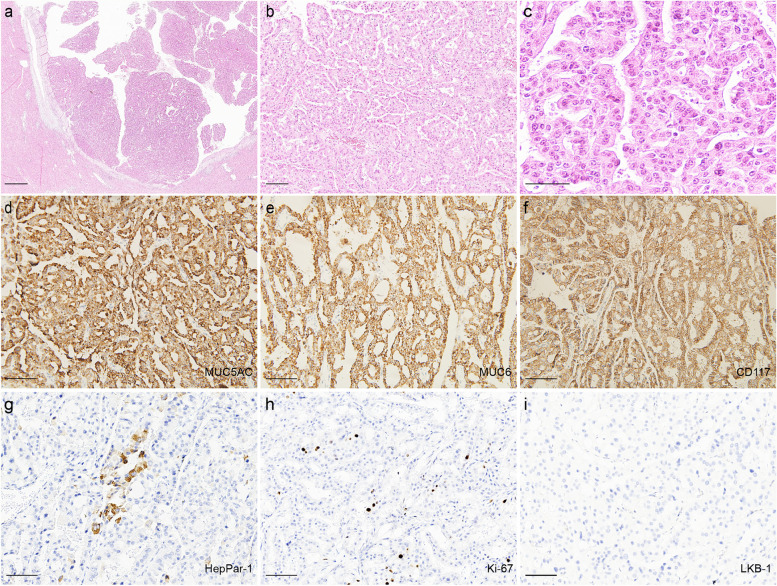
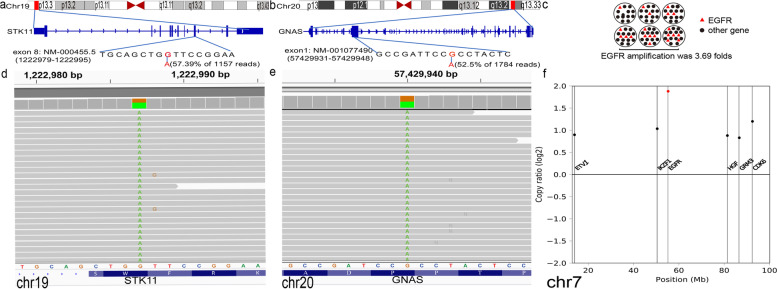
Case presentation: We herein describe the case of a 44-year-old woman who presented as polyps in the intestinal lumen of sigmoid colon and a 3.1 × 2.1 cm mass in the left lobe of liver. Gross feature revealed a cystic papillary mass and the neoplasm had a clear boundary with the surrounding liver tissue. Histology revealed complex papillary structures, a small amount of fine fibrovascular cores and immunohistochemistry showed extensive positive for MUC5AC, MUC6, CD117. Therefore, histological and immunohistochemical examination of the liver tumor suggested the diagnosis of IOPN. Next-generation sequencing (NGS) revealed other than STK11 germline mutation, the tumor also harbors GNAS somatic mutation at codon 478 and EGFR amplification.
Conclusion: To our knowledge, this is the first report of IOPN arising in PJS. This case enlarges the spectrum of PJS related tumors and genetic rearrangements in IOPN.
Keywords: EGFR; GNAS; Intraductal oncocytic papillary neoplasm; Peutz-Jeghers syndrome; STK11.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
STK11/LKB1 Peutz-Jeghers gene inactivation in intraductal papillary-mucinous neoplasms of the pancreas.Am J Pathol. 2001 Dec;159(6):2017-22. doi: 10.1016/S0002-9440(10)63053-2. Am J Pathol. 2001. PMID: 11733352 Free PMC article.
-
Intraductal papillary neoplasm of the bile duct: a biliary equivalent to intraductal papillary mucinous neoplasm of the pancreas?Hepatology. 2012 Oct;56(4):1352-60. doi: 10.1002/hep.25786. Epub 2012 Aug 27. Hepatology. 2012. PMID: 22504729
-
Clinicopathological features of intraductal papillary neoplasms of the bile duct: a comparison with intraductal papillary mucinous neoplasm of the pancreas with reference to subtypes.Virchows Arch. 2017 Jul;471(1):65-76. doi: 10.1007/s00428-017-2144-9. Epub 2017 May 26. Virchows Arch. 2017. PMID: 28550497
-
Intraductal Papillary Neoplasm of Bile Duct: Updated Clinicopathological Characteristics and Molecular and Genetic Alterations.J Clin Med. 2020 Dec 9;9(12):3991. doi: 10.3390/jcm9123991. J Clin Med. 2020. PMID: 33317146 Free PMC article. Review.
-
Intraductal papillary neoplasm of the bile duct: review of updated clinicopathological and imaging characteristics.Br J Surg. 2023 Aug 11;110(9):1229-1240. doi: 10.1093/bjs/znad202. Br J Surg. 2023. PMID: 37463281 Review.
Cited by
-
Understanding the Genetic Landscape of Pancreatic Ductal Adenocarcinoma to Support Personalized Medicine: A Systematic Review.Cancers (Basel). 2023 Dec 21;16(1):56. doi: 10.3390/cancers16010056. Cancers (Basel). 2023. PMID: 38201484 Free PMC article. Review.
-
A missed case of intraductal oncocytic papillary neoplasm associated with missed stones in extrahepatic bile duct: a case report.Front Oncol. 2024 May 21;14:1349914. doi: 10.3389/fonc.2024.1349914. eCollection 2024. Front Oncol. 2024. PMID: 38841165 Free PMC article.
References
-
- Boland CR, Idos GE, Durno C, Giardiello FM, Anderson JC, Burke CA, et al. Diagnosis and management of Cancer Risk in the gastrointestinal hamartomatous polyposis syndromes: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2022;162:2063–85. doi: 10.1053/j.gastro.2022.02.021. - DOI - PubMed
-
- Yang CY, Huang WJ, Tsai JH, Cheng A, Chen CC, Hsu HP, et al. Targeted next-generation sequencing identifies distinct clinicopathologic and molecular entities of intraductal papillary neoplasms of the bile duct. Mod pathology: official J United States Can Acad Pathol Inc. 2019;32:1637–45. doi: 10.1038/s41379-019-0306-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
