

Affinity purification of serum-derived anti-IA-2 autoantibodies in type 1 diabetes using a novel MBP-IA-2 fusion protein
- PMID: 36578528
- PMCID: PMC9791830
- DOI: 10.1016/j.bbrep.2022.101413
Affinity purification of serum-derived anti-IA-2 autoantibodies in type 1 diabetes using a novel MBP-IA-2 fusion protein
Abstract
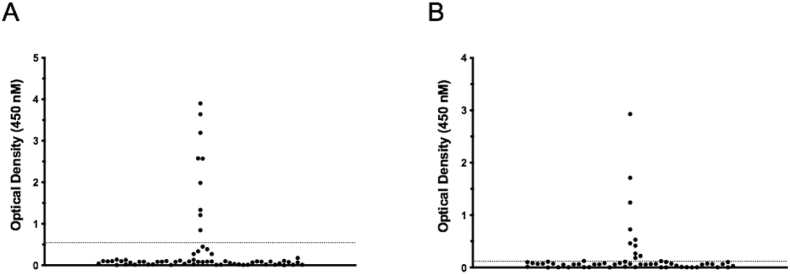
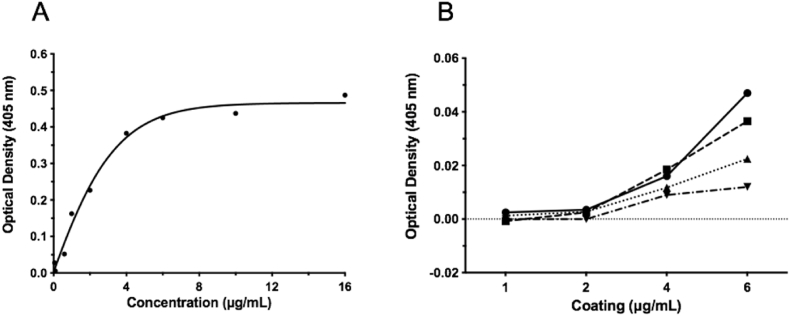
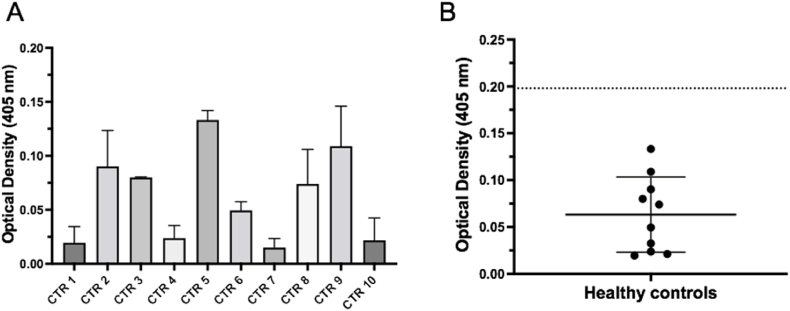
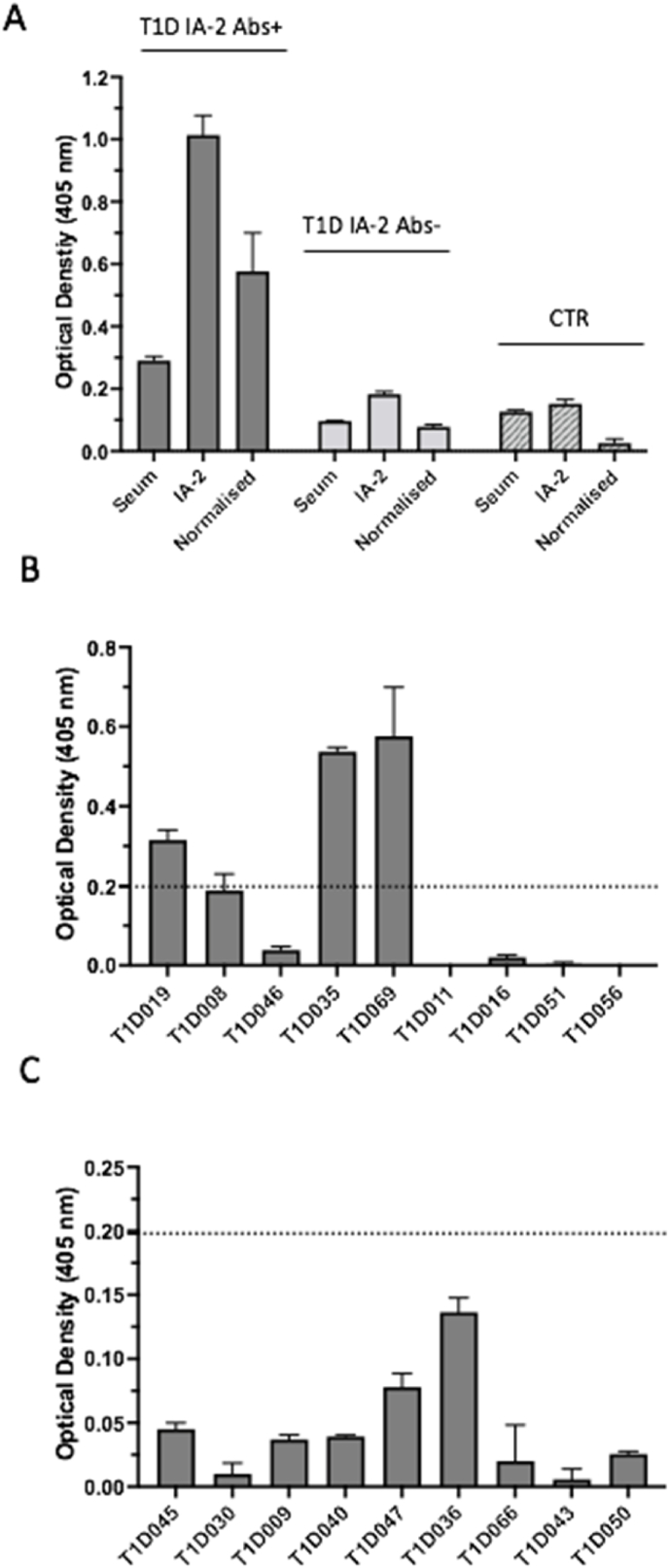
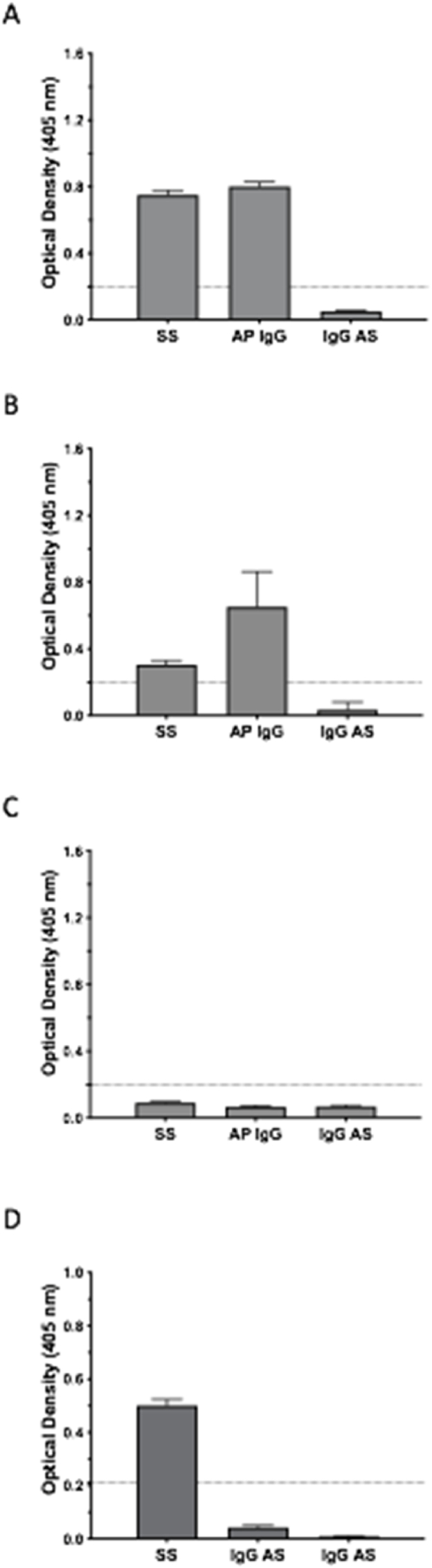
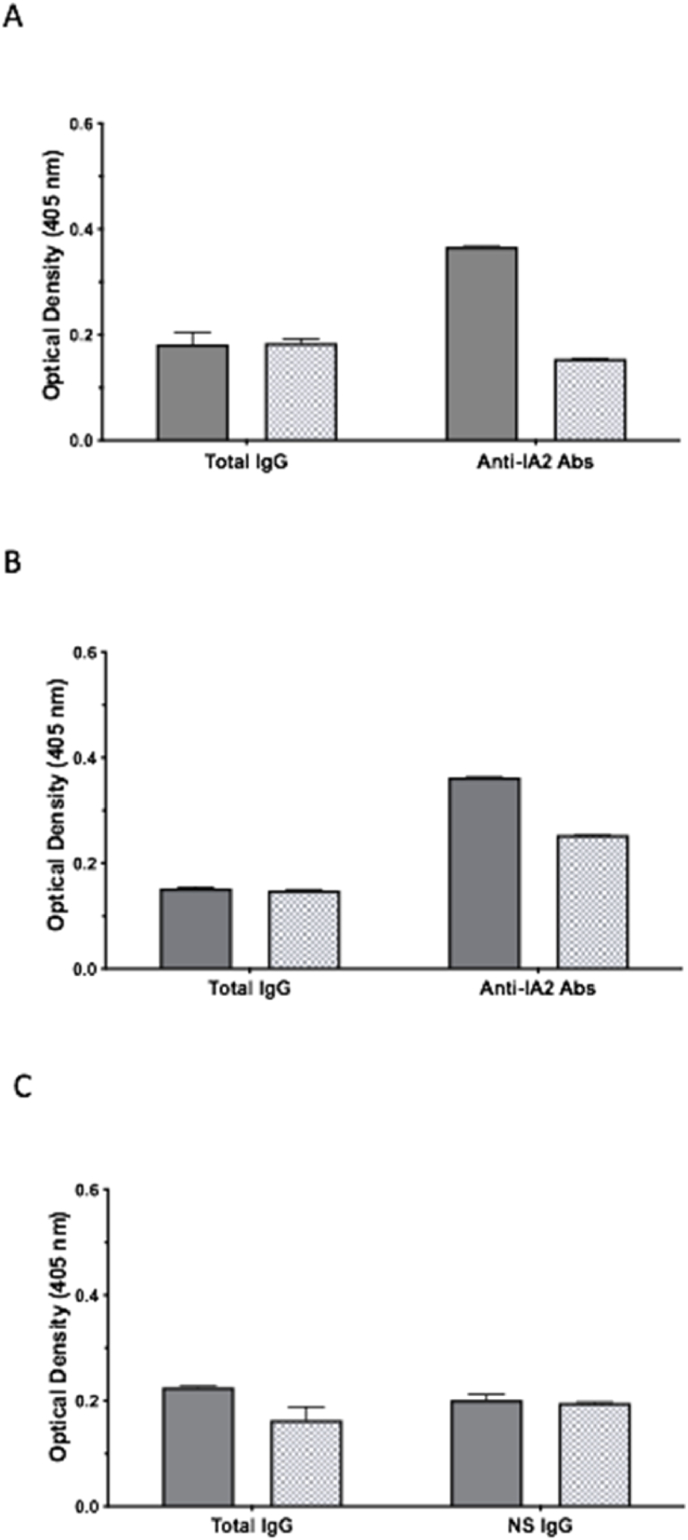
Autoantibodies targeting epitopes contained within the intracellular domain (IC) of the protein phosphatase-like islet antigen 2 (IA-2) are a common marker of autoimmune type 1 diabetes (T1D), however the isolation of genuine, serum derived anti-IA-2 autoantibodies has proven challenging due to a lack of suitable bioassays. In the current study, an ELISA format was developed for affinity purification of human anti-IA-2ic autoantibodies utilizing a fusion protein (FP) incorporating maltose binding protein and the full-length IA-2IC domain. Using a T1D patient cohort validated for anti-IA-2ic autoantibodies by commercial ELISA, we demonstrate the MBP-IA-2ic FP ELISA detects serum anti-IA-2IC autoantibodies from 3 of 9 IA-2 positive patients. Further to this, a multi-plate MBP-IA-2ic FP ELISA protocol specifically affinity purifies IgG enriched for anti-IA-2ic autoantibodies. Interestingly, serum derived autoantibodies immobilised on the MBP-IA-2ic FP ELISA demonstrate increased Kappa light chain usage when compared to the respective total IgG derived from donor patients, suggesting a clonally restricted repertoire of anti-IA-2ic autoantigen specific B plasma cells is responsible for autoantibodies detect by the MBP-IA-2ic FP ELISA. This study is the first to demonstrate the generation of specific, genuine human derived anti-IA-2ic autoantibodies, thereby facilitating further investigation into the origin and functional significance of IA-2 autoantibodies in T1D.
Keywords: Affinity purification; Autoantibodies; Clonal restriction; FP, fusion protein; GAD65, glutamic acid decarboxylase 65; IA-2; IA-2, islet antigen 2; IC, intracellular; OD, optical density; T1D, Type 1 Diabetes; Type 1 diabetes; β, beta cell.
© 2022 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
