

Efficacy and Safety of Semaglutide for Weight Loss in Obesity Without Diabetes: A Systematic Review and Meta-Analysis
- PMID: 36578889
- PMCID: PMC9758543
- DOI: 10.15605/jafes.037.02.14
Efficacy and Safety of Semaglutide for Weight Loss in Obesity Without Diabetes: A Systematic Review and Meta-Analysis
Abstract
Background: The weight loss benefit of semaglutide in patients with diabetes is well-documented, but its clinical utility in treating obesity among patients without diabetes is less described. We therefore assessed the efficacy and safety of subcutaneous semaglutide as treatment for obesity in patients without diabetes.
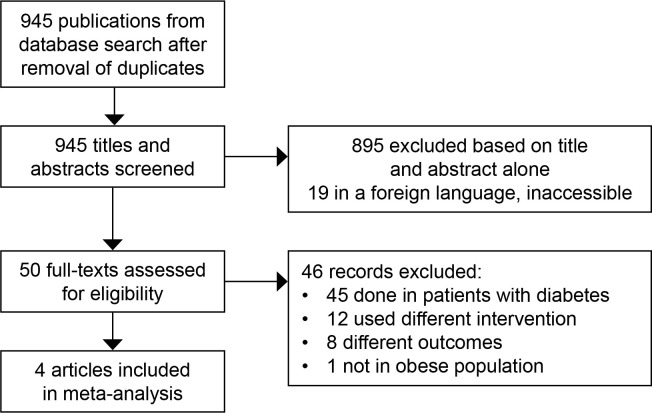
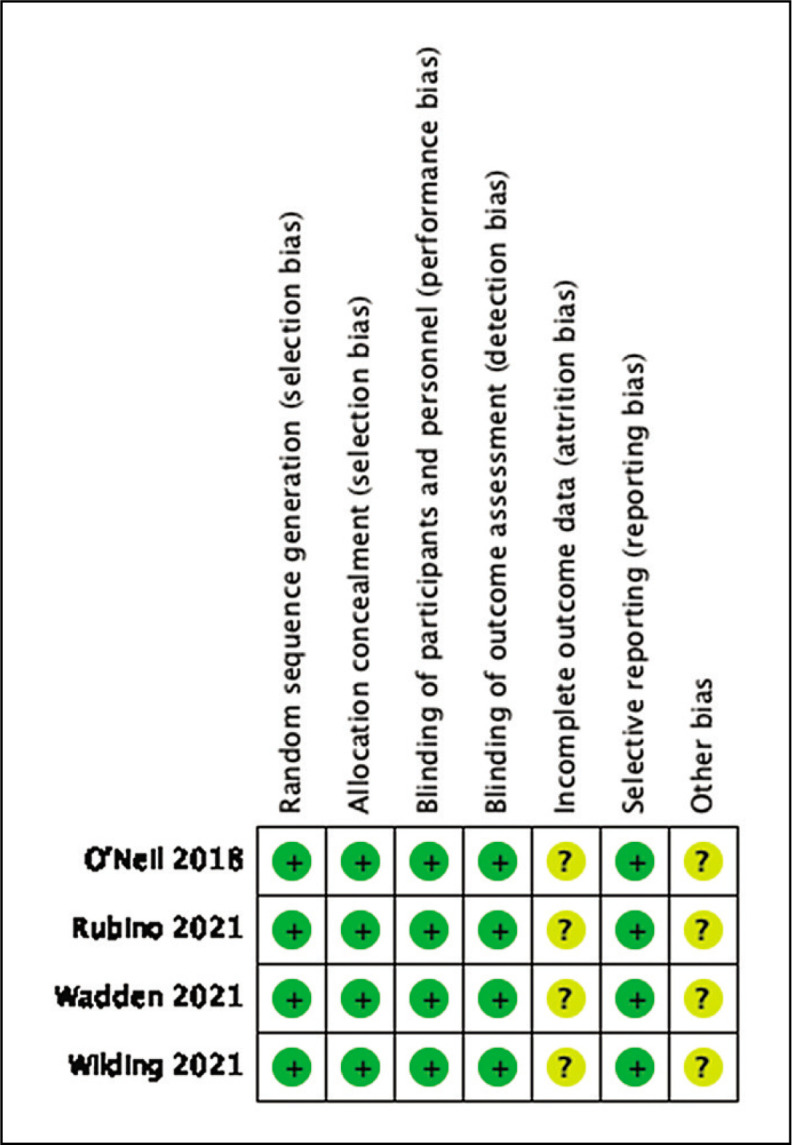
Methodology: A comprehensive search of PubMed/MEDLINE, Cochrane and Google scholar was performed to identify trials on the efficacy and safety of subcutaneous semaglutide on patients with obesity without diabetes. Primary outcome was expressed as percent mean weight difference. Secondary outcomes including risk for gastrointestinal adverse events, discontinuation of treatment and serious adverse events were expressed as risk ratios. These were calculated using the random effects model.
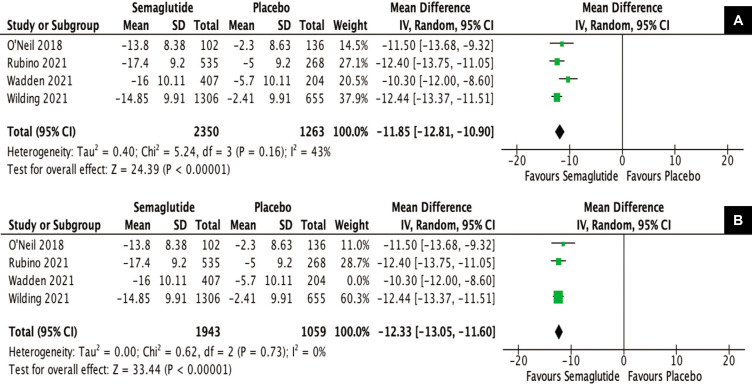
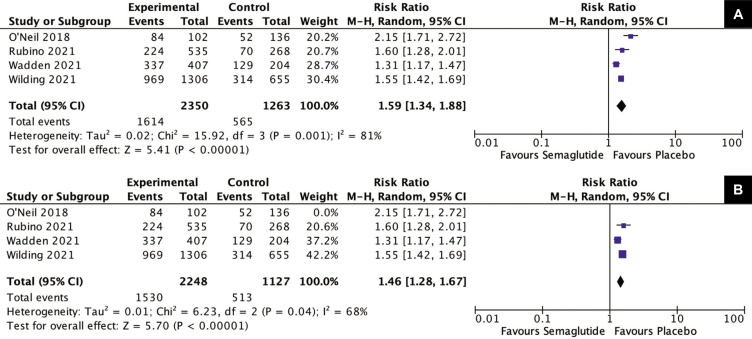
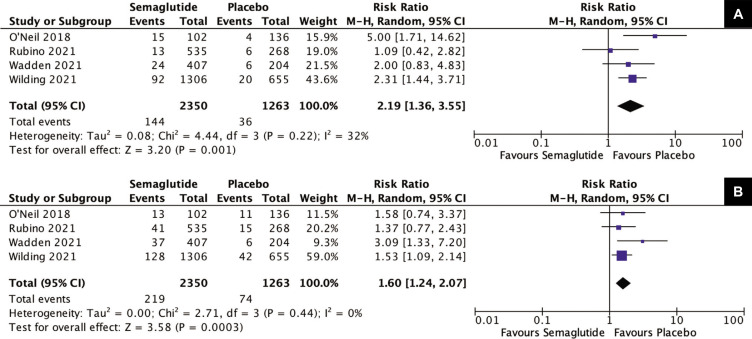
Results: The study included 4 randomized controlled trials having a total of 3,613 individuals with obesity without diabetes. The mean difference for weight reduction was -11.85%, favoring semaglutide [95% confidence interval (CI) (-12.81,-10.90), p<0.00001]. Secondary outcomes showed that the risk of developing gastrointestinal adverse events was 1.59 times more likely with semaglutide (RR 1.59, 95%CI [1.34, 1.88], p<0.00001). Risk for discontinuation due to adverse events was twice as likely in the semaglutide group (RR 2.19, 95%CI [1.36,3.55], p=0.001) and the risk for serious adverse events was 1.6 times more likely for semaglutide (RR1.60, 95%CI [1.24, 2.07], p=0.0003). Serious events were mostly of gastrointestinal and hepatobiliary disorders such as acute pancreatitis and cholelithiasis.
Conclusion: Among individuals with obesity without type 2 diabetes, subcutaneous semaglutide is effective for weight loss with an 11.85% reduction from baseline compared to placebo. This supports the use of semaglutide for weight management in obesity. However, risk of gastrointestinal adverse events, discontinuation of treatment and serious adverse events were higher in the semaglutide group versus placebo.
Keywords: Glucagon-like Peptide -1; obesity; semaglutide; weight loss.
© 2022 Journal of the ASEAN Federation of Endocrine Societies.
Conflict of interest statement
OAD reports receiving consulting fees from Eli Lilly and Novo Nordisk for service outside the submitted work, as well as honoraria for speaking engagements from Astra Zeneca, Novo Nordisk, and Eli Lilly outside the submitted work. HCT and MMM declare no conflict of interest in association with this study.
Figures
Similar articles
-
Long-Term Efficacy and Safety of Once-Weekly Semaglutide for Weight Loss in Patients Without Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Am J Cardiol. 2024 Jul 1;222:121-130. doi: 10.1016/j.amjcard.2024.04.041. Epub 2024 Apr 26. Am J Cardiol. 2024. PMID: 38679221
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Metformin for women who are overweight or obese during pregnancy for improving maternal and infant outcomes.Cochrane Database Syst Rev. 2018 Jul 24;7(7):CD010564. doi: 10.1002/14651858.CD010564.pub2. Cochrane Database Syst Rev. 2018. PMID: 30039871 Free PMC article.
-
Efficacy and safety of once-weekly subcutaneous semaglutide on weight loss in patients with overweight or obesity without diabetes mellitus-A systematic review and meta-analysis of randomized controlled trials.Obes Rev. 2024 Sep;25(9):e13792. doi: 10.1111/obr.13792. Epub 2024 Jun 23. Obes Rev. 2024. PMID: 38923272
-
Immunosuppressive treatment for primary membranous nephropathy in adults with nephrotic syndrome.Cochrane Database Syst Rev. 2021 Nov 15;11(11):CD004293. doi: 10.1002/14651858.CD004293.pub4. Cochrane Database Syst Rev. 2021. PMID: 34778952 Free PMC article.
Cited by
-
Flavonoids as Potential Modulators of Pancreatic Lipase Catalytic Activity.Pharmaceutics. 2025 Jan 25;17(2):163. doi: 10.3390/pharmaceutics17020163. Pharmaceutics. 2025. PMID: 40006530 Free PMC article.
-
Exploring Glucagon-Like Peptide-1 Receptor Agonists Usage Among Non-Diabetic Healthcare Providers: A Cross-Sectional Multi-Country Study.Health Sci Rep. 2025 Apr 23;8(4):e70638. doi: 10.1002/hsr2.70638. eCollection 2025 Apr. Health Sci Rep. 2025. PMID: 40276133 Free PMC article.
-
Efficacy of Glucagon-Like Peptide 1 (GLP-1) Receptor Agonists for Weight Loss Management in Non-Diabetic Patients.Cureus. 2024 Jul 21;16(7):e65050. doi: 10.7759/cureus.65050. eCollection 2024 Jul. Cureus. 2024. PMID: 39165448 Free PMC article. Review.
-
Depression and Obesity-Do We Know Everything about It? A Narrative Review.Nutrients. 2024 Oct 4;16(19):3383. doi: 10.3390/nu16193383. Nutrients. 2024. PMID: 39408350 Free PMC article. Review.
-
Effectiveness and safety of semaglutide in overweight/obese adults with or without type 2 diabetes: A systematic review and meta-analysis.J Res Med Sci. 2024 Sep 30;29:60. doi: 10.4103/jrms.jrms_693_23. eCollection 2024. J Res Med Sci. 2024. PMID: 39629036 Free PMC article. Review.
References
-
- World Health Organization . Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesityand-overweight. Accessed 15 May 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical