

Derivation and validation of a clinical decision rule to risk-stratify COVID-19 patients discharged from the emergency department: The CCEDRRN COVID discharge score
- PMID: 36579029
- PMCID: PMC9780419
- DOI: 10.1002/emp2.12868
Derivation and validation of a clinical decision rule to risk-stratify COVID-19 patients discharged from the emergency department: The CCEDRRN COVID discharge score
Abstract
Objective: To risk-stratify COVID-19 patients being considered for discharge from the emergency department (ED).
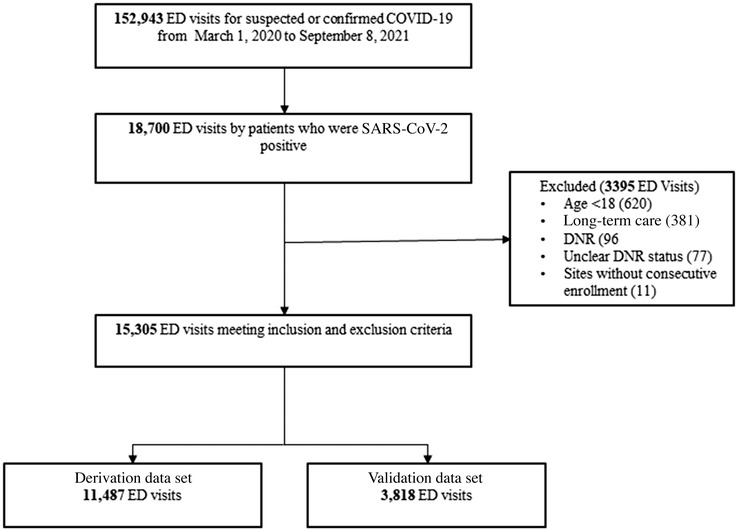
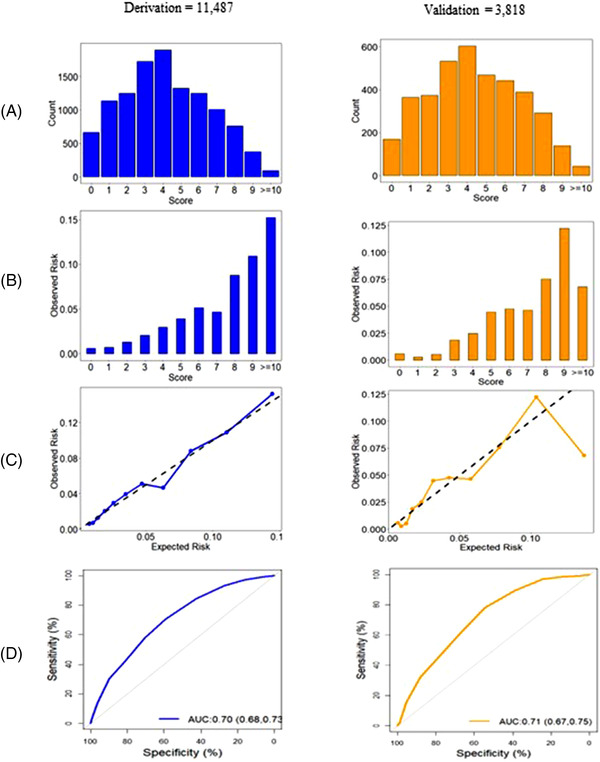
Methods: We conducted an observational study to derive and validate a clinical decision rule to identify COVID-19 patients at risk for hospital admission or death within 72 hours of ED discharge. We used data from 49 sites in the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN) between March 1, 2020, and September 8, 2021. We randomly assigned hospitals to derivation or validation and prespecified clinical variables as candidate predictors. We used logistic regression to develop the score in a derivation cohort and examined its performance in predicting short-term adverse outcomes in a validation cohort.
Results: Of 15,305 eligible patient visits, 535 (3.6%) experienced the outcome. The score included age, sex, pregnancy status, temperature, arrival mode, respiratory rate, and respiratory distress. The area under the curve was 0.70 (95% confidence interval [CI] 0.68-0.73) in derivation and 0.71 (95% CI 0.68-0.73) in combined derivation and validation cohorts. Among those with a score of 3 or less, the risk for the primary outcome was 1.9% or less, and the sensitivity of using 3 as a rule-out score was 89.3% (95% CI 82.7-94.0). Among those with a score of ≥9, the risk for the primary outcome was as high as 12.2% and the specificity of using 9 as a rule-in score was 95.6% (95% CI 94.9-96.2).
Conclusion: The CCEDRRN COVID discharge score can identify patients at risk of short-term adverse outcomes after ED discharge with variables that are readily available on patient arrival.
Keywords: COVID‐19; clinical decision instrument; clinical prediction score; coronavirus disease; emergency medicine; prediction model.
© 2022 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors have declared no conflict of interest.
Figures
Similar articles
-
The CCEDRRN COVID-19 Mortality Score to predict death among nonpalliative patients with COVID-19 presenting to emergency departments: a derivation and validation study.CMAJ Open. 2022 Feb 8;10(1):E90-E99. doi: 10.9778/cmajo.20210243. Print 2022 Jan-Mar. CMAJ Open. 2022. PMID: 35135824 Free PMC article.
-
CCEDRRN COVID-19 Infection Score (CCIS): development and validation in a Canadian cohort of a clinical risk score to predict SARS-CoV-2 infection in patients presenting to the emergency department with suspected COVID-19.BMJ Open. 2021 Dec 2;11(12):e055832. doi: 10.1136/bmjopen-2021-055832. BMJ Open. 2021. PMID: 34857584 Free PMC article.
-
Predictive score for mortality in patients with COPD exacerbations attending hospital emergency departments.BMC Med. 2014 Apr 23;12:66. doi: 10.1186/1741-7015-12-66. BMC Med. 2014. PMID: 24758312 Free PMC article.
-
Derivation of a Clinical Risk Score to Predict 14-Day Occurrence of Hypoxia, ICU Admission, and Death Among Patients with Coronavirus Disease 2019.J Gen Intern Med. 2021 Mar;36(3):730-737. doi: 10.1007/s11606-020-06353-5. Epub 2020 Dec 3. J Gen Intern Med. 2021. PMID: 33274414 Free PMC article.
-
Can I Send This Syncope Patient Home From the Emergency Department?J Emerg Med. 2021 Dec;61(6):801-809. doi: 10.1016/j.jemermed.2021.07.060. Epub 2021 Sep 15. J Emerg Med. 2021. PMID: 34535304 Review.
Cited by
-
Comparing methods to classify admitted patients with SARS-CoV-2 as admitted for COVID-19 versus with incidental SARS-CoV-2: A cohort study.PLoS One. 2023 Sep 26;18(9):e0291580. doi: 10.1371/journal.pone.0291580. eCollection 2023. PLoS One. 2023. PMID: 37751455 Free PMC article.
-
A systematic review of tools for predicting complications in patients with influenza-like illness.Heliyon. 2023 Dec 3;10(1):e23227. doi: 10.1016/j.heliyon.2023.e23227. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38163091 Free PMC article. Review.
-
The response of Canada's clinical health research ecosystem to the COVID-19 pandemic.CMAJ. 2024 Jun 16;196(23):E779-E788. doi: 10.1503/cmaj.230760. CMAJ. 2024. PMID: 38885975 Free PMC article.
-
Accuracy of the Canadian COVID-19 Mortality Score (CCMS) to predict in-hospital mortality among vaccinated and unvaccinated patients infected with Omicron: a cohort study.BMJ Open. 2024 Nov 19;14(11):e083280. doi: 10.1136/bmjopen-2023-083280. BMJ Open. 2024. PMID: 39566942 Free PMC article.
References
-
- Hohl CM, Rosychuk RJ, Hau JP, et al. Treatments, resource utilization, and outcomes of COVID‐19 patients presenting to emergency departments across pandemic waves: an observational study by the Canadian COVID‐19 emergency department rapid response network (CCEDRRN). Can J Emerg Med. 2022. doi: 10.1007/s43678-022-00275-3 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources