

Clinical and Virological Characteristics and Prognostic Factors in Viral Necrotizing Retinitis
- PMID: 36579507
- PMCID: PMC9695359
- DOI: 10.3390/jpm12111785
Clinical and Virological Characteristics and Prognostic Factors in Viral Necrotizing Retinitis
Abstract
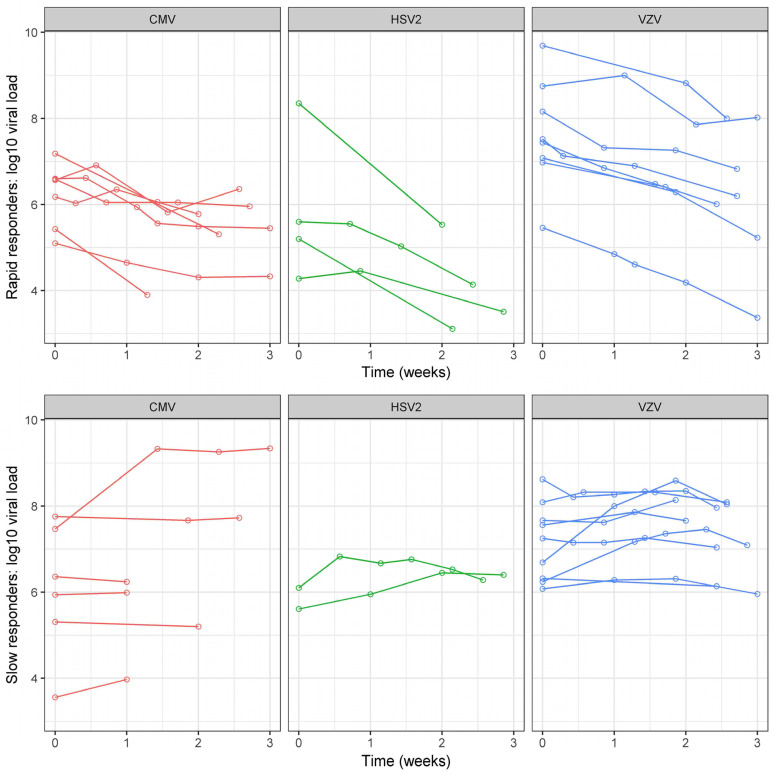
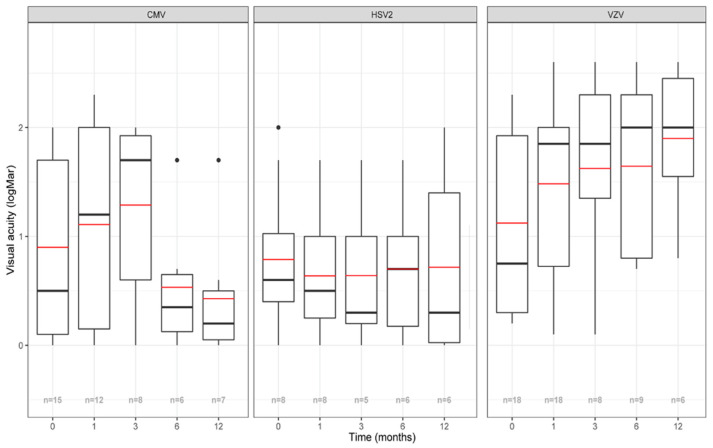
Purpose: Describe the clinical and virological characteristics of viral necrotizing retinitis (VNR) and assess its prognostic factors. Methods: Retrospective study (Pitié Salpêtrière Hospital, Paris) of consecutive VNR patients diagnosed and monitored by qPCR on aqueous humor between 2015 and 2019. All patients received induction therapy with intravenous +/− intravitreal injections (IVI) of antivirals. Results: Forty-one eyes of 37 patients with a mean age of 56 years were included. Involved viruses were VZV (44%), CMV (37%) and HSV2 (19%). Acute retinal necrosis represented 51%, progressive outer retinal necrosis 12% and CMV retinitis 37% of eyes. Forty-six percent of patients were immunocompromised. Median BCVA was 0.7 LogMAR at baseline and 0.8 LogMAR after an average of 14.1 months. VNR bilateralized in 27% of cases after 32 months. Retinal detachment (RD) occurred in 27% of cases after a mean duration of 98 days. Factors associated with a “poor BCVA” at 1 month were: advanced age, low baseline BCVA, high vitritis grade and viral load (VL) at baseline and the “slow responder” status (i.e., VL decrease <50% after 2 weeks of treatment). Factors associated with RD were: advanced age, immunocompetence, low baseline BCVA, high vitritis grade at baseline and use of ≤5 IVIs. Conclusions: Clinical factors including advanced age, immunocompetence, low BCVA and high vitritis grade at baseline were associated with a poor prognosis. New virological factors were predictive of a poor outcome: high baseline VL and the “slow responder” status. Sequential intraocular fluid sampling might help prognosticate the outcomes of VNR.
Keywords: CMV; HSV; VZV; outcome; prognosis; retinal detachment; viral load; viral necrotizing retinitis.
Conflict of interest statement
S.T. received consultant and lecture fees from Novartis, Horus Pharma, Allergan and Bayer outside the submitted work. B.B. reports consultant fees from Théa, Novartis, Bayer, Allergan-Abbvie, Alimera and Santen outside the submitted work.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
