

Predictors of Successful Medical Management With Methotrexate in Unruptured Tubal Ectopic Pregnancy
- PMID: 36580082
- PMCID: PMC9792717
- DOI: 10.7759/cureus.31923
Predictors of Successful Medical Management With Methotrexate in Unruptured Tubal Ectopic Pregnancy
Abstract
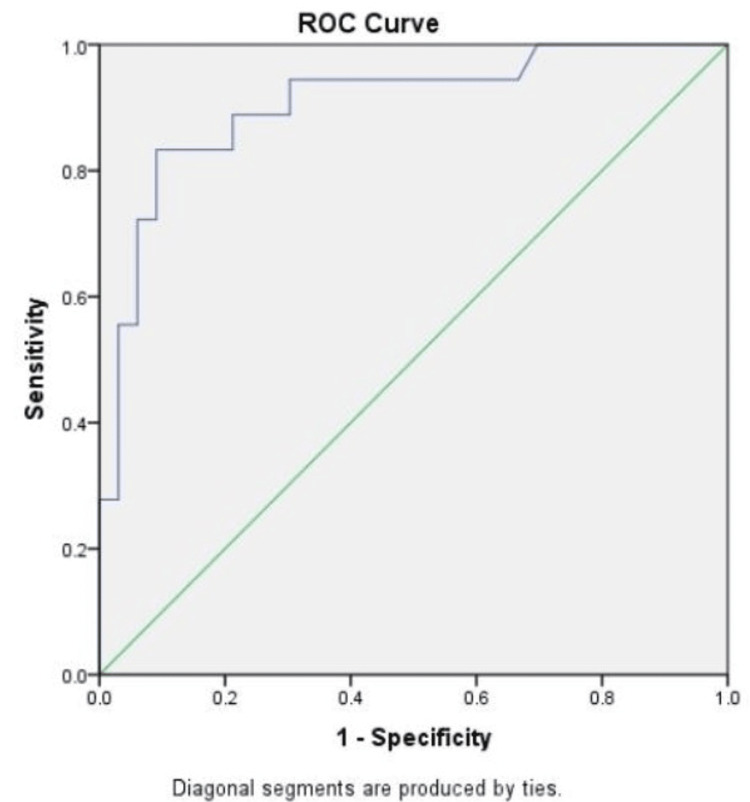
Introduction Medical treatment with methotrexate (MTX) is a safe and effective alternative to surgery in carefully selected cases of ectopic pregnancies diagnosed early prior to rupture. Aim To determine the optimal pre-treatment levels of beta human chorionic gonadotropin (𝛽-hCG) and its changing trends most likely to have a successful outcome with medical management. Material and methods A prospective observational study was conducted in a tertiary teaching hospital from December 2018 to May 2021. "Single-dose" MTX regime was used for medical management of ectopic pregnancy in patients fulfilling the selection criteria. The 𝛽-hCG levels were recorded at baseline and on day 4 and day 7 of MTX injection. Thereafter, at weekly intervals till complete resolution or surgical intervention due to failure of medical management. In addition, receiver operating characteristic (ROC) curve analysis for a pre-treatment 𝛽-hCG cut-off value and changing trends in post-treatment 𝛽- hCG levels most likely to have a successful outcome with MTX treatment were determined. Results Fifty patients fulfilling the inclusion criteria were included in the study, with successful medical management in 33 (66%). The mean pre-treatment 𝛽-hCG levels in women with successful medical management were 3270.97 (+/- 901) compared to 5249.17 (+/-808.02) for those with treatment failure (p=0.00001). The mean 𝛽-hCG level in the failed treatment group was significantly higher on day 4 than the pre-treatment levels (6742.56 +/- 572 vs. 5249.17+/- 808.02; p<0.05). Inadequate reduction of 𝛽-hCG level on day 7 (<15% of day 4 levels) requiring repeat dosage of MTX was more likely to have an unsuccessful outcome (p=0.00001). The area under curve (AUC) value of 0.905 (95% CI: 0.814-0.996) depicted that pre-treatment 𝛽-hCG level of 4000 mIU/ml taken as the cut-off value was able to predict levels ≤4000 mIU/ml had a greater likelihood of successful outcome with MTX, having a sensitivity of 84.5%, specificity of 83.3%, positive predictive value (PPV) of 90.3%, and negative predictive value (NPV) of 75% (p< 0.05). Demographic variables or previous clinical history, considered risk factors for ectopic pregnancy, did not affect the outcome of medical management in this study. Conclusion Medical management of ectopic pregnancy is a viable first-line treatment option in carefully selected patients. In this study, the most important predictors for the successful outcome of medical management were the pre-treatment β-hCG levels and their fall on day 4 and day 7 after MTX therapy.
Keywords: methotrexate; receiver operating characteristic (roc) analysis; serum beta hcg; successful treatment outcome; unruptured tubal ectopic pregnancy.
Copyright © 2022, Ray et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira N. Hum Reprod. 2002;17:3224–3230. - PubMed
-
- A clinical analysis of ectopic pregnancies in a tertiary care hospital in Hyderabad. Pranathi L, Madhavi Y. Asian Pac J Health Sci. 2018;5:20–24.
-
- A clinical study of trends of ectopic pregnancy and its management in a tertiary care hospital. Puttaraju CM, Nagendraprasad N, Sailakshmi MP. Int J Reprod Contracept Obstet Gynecol. 2019;8:4834–4841.
-
- Medical treatment of ectopic pregnancy: a committee opinion. Practice Committee of American Society for Reproductive Medicine. http://dx.doi.org/10.1016/j.fertnstert.2013.06.013. Fertil Steril. 2013;100:638–644. - PubMed
-
- The use of a new logistic regression model for predicting the outcome of pregnancies of unknown location. Condous G, Okaro E, Khalid A, et al. Hum Reprod. 2004;19:1900–1910. - PubMed
LinkOut - more resources
Full Text Sources