

Myocardial infarction after craniotomy for asymptomatic meningioma
- PMID: 36581354
- PMCID: PMC9806024
- DOI: 10.1136/bcr-2022-252256
Myocardial infarction after craniotomy for asymptomatic meningioma
Abstract
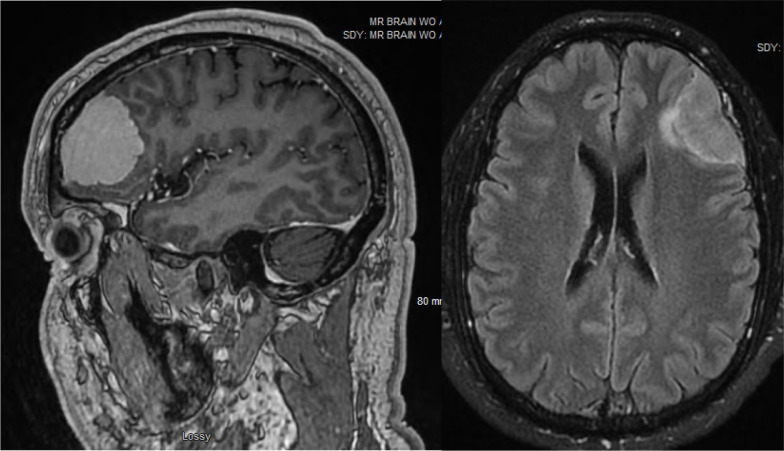
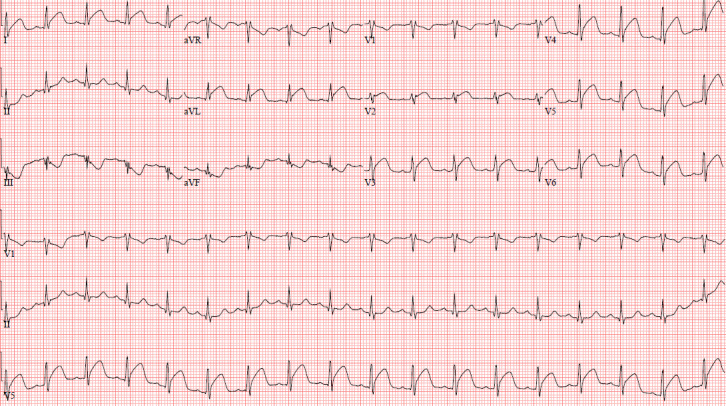
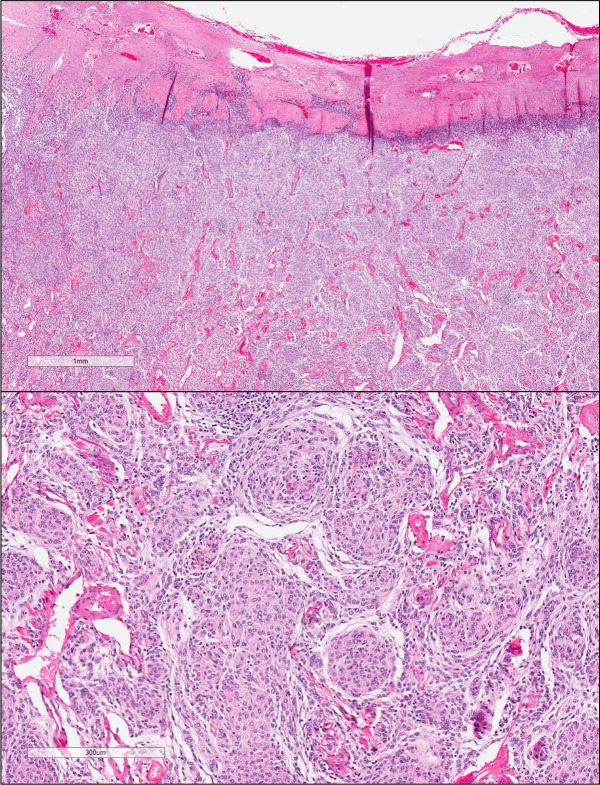
A man in his 40s with a history of coronary artery disease previously treated with a drug-eluting stent presented for elective craniotomy and resection of an asymptomatic but enlarging meningioma. During his craniotomy, he received desmopressin and tranexamic acid for surgical bleeding. Postoperatively, the patient developed chest pain and was found to have an ST-elevation myocardial infarction (MI). Because of the patient's recent neurosurgery, standard post-MI care was contraindicated and he was instead managed symptomatically in the intensive care unit. Echocardiogram on postoperative day 1 demonstrated no regional wall motion abnormalities and an ejection fraction of 60%. His presentation was consistent with thrombosis of his diagonal stent. He was transferred out of the intensive care unit on postoperative day 1 and discharged home on postoperative day 3.
Keywords: Adult intensive care; Drug therapy related to surgery; Ischaemic heart disease; Neurosurgery; Unwanted effects / adverse reactions.
© BMJ Publishing Group Limited 2022. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical