

Electroanatomical mapping-guided left bundle branch area pacing in patients with structural heart disease and advanced conduction abnormalities
- PMID: 36581450
- PMCID: PMC10062301
- DOI: 10.1093/europace/euac232
Electroanatomical mapping-guided left bundle branch area pacing in patients with structural heart disease and advanced conduction abnormalities
Abstract
Aims: Left bundle branch area pacing (LBBAP) can be technically challenging and fluoroscopy-intense. Three-dimensional electroanatomical mapping (EAM) facilitates non-fluoroscopic lead navigation and electrogram mapping. We sought to prospectively evaluate the feasibility, safety, and outcomes of routine EAM-guided LBBAP in patients with structural heart disease (SHD) and advanced conduction abnormalities.
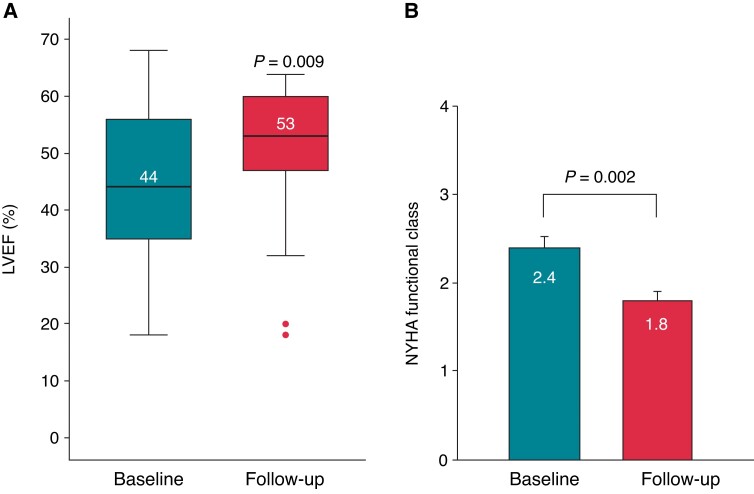
Methods and results: Consecutive patients with SHD and conduction abnormalities who underwent an attempt at EAM-guided LBBAP were included. The feasibility, safety, procedural, and mid-term outcomes were evaluated. Electrical, echocardiographic, and clinical parameters were assessed at implantation and last follow-up. Thirty-two patients (68 ± 18 years; 19% female) were included, of which 75% had intrinsic QRS > 150 ms, 53% left bundle branch block, and 25% right bundle branch block. Primary EAM-guided LBBAP was successful in 29 patients (91%). The procedural duration was 95 (70-110) min, total fluoroscopy time 0.93 (0.40-1.73) min, and total fluoroscopy dose 35.4 (20.5-77.2) cGy cm2. Paced QRS duration (QRSd) was significantly shorter than intrinsic QRSd (121.9 ± 10.7 vs. 159.2 ± 34.4 ms; P < 0.001) and remained stable during the mean follow-up of 7.0 ± 5.9 months. The LBBAP capture threshold was 0.57 ± 0.23 V/0.4 ms at implantation and remained low during follow-up (0.58 ± 0.18 V/0.5 ± 0.2 ms; P = 0.877). Overall left ventricular ejection fraction improved significantly from 44.2 ± 14.3% at baseline to 49.4 ± 13.1% at follow-up (P = 0.009), New York Heart Association class from 2.4 ± 0.6 to 1.8 ± 0.6 (P = 0.002), respectively. No complications occurred that required intervention.
Conclusion: Routine near-zero fluoroscopy EAM-guided LBBAP can safely be performed in patients with SHD and advanced conduction abnormalities with high success rates and favourable mid-term outcomes. Further studies are needed to investigate whether the use of EAM improves the overall outcome of conduction system pacing and to identify specific patient populations who benefit the most from EAM-guided lead implantation.
Keywords: Cardiac implantable electronic device; Electroanatomical mapping; Implantation technique; Left bundle branch area pacing; Radiation exposure.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: S.R. is a consultant for Medtronic and a member of the Medtronic European Conduction System Advisory Board; he has received speaker honoraria and proctor fees from Abbott, Biotronik, and Medtronic to his institution without personal financial benefits. D.S. is an employee of Abbott. G.H. has received research grants from Abbott and Boston Scientific to his institution without personal financial benefits. The remaining authors have declared no conflicts of interest.
Figures




References
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IMet al. . 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Europace 2022;24:71–164. - PubMed
-
- Vijayaraman P, Ponnusamy S, Cano Ó, Sharma PS, Naperkowski A, Subsposh FA et al. . Left bundle branch area pacing for cardiac resynchronization therapy: results from the international LBBAP collaborative study group. JACC Clin Electrophysiol 2021;7:135–47. - PubMed
-
- Tops LF, Schalij MJ, Bax JJ. The effects of right ventricular apical pacing on ventricular function and dyssynchrony: implications for therapy. J Am Coll Cardiol 2009:764–76. - PubMed
-
- Huang W, Su L, Wu S, Xu L, Xiao F, Zhou X et al. . Long-term outcomes of His bundle pacing in patients with heart failure with left bundle branch block. Heart 2019;105:137–43. - PubMed
-
- Sharma PS, Huang HD, Trohman RG, Naperkowski A, Ellenbogen KA, Vijayaraman P. Low fluoroscopy permanent His bundle pacing using electroanatomic mapping: a feasibility study. Circ Arrhythm Electrophysiol 2019;12:e006967. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
