

Three-dimensional cephalometric outcome predictability of virtual orthodontic-surgical planning in surgery-first approach
- PMID: 36581697
- PMCID: PMC9800679
- DOI: 10.1186/s40510-022-00448-x
Three-dimensional cephalometric outcome predictability of virtual orthodontic-surgical planning in surgery-first approach
Abstract
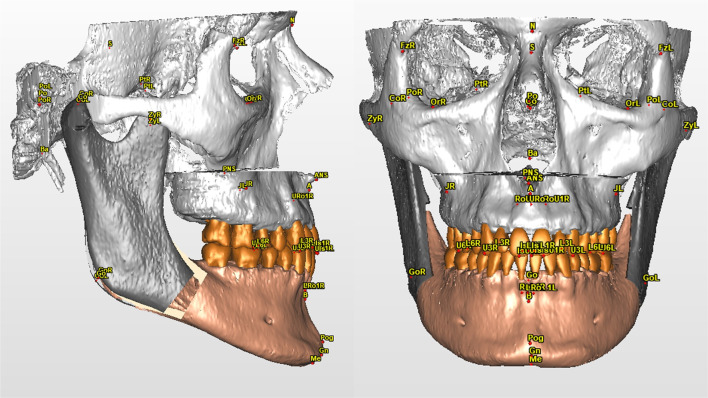
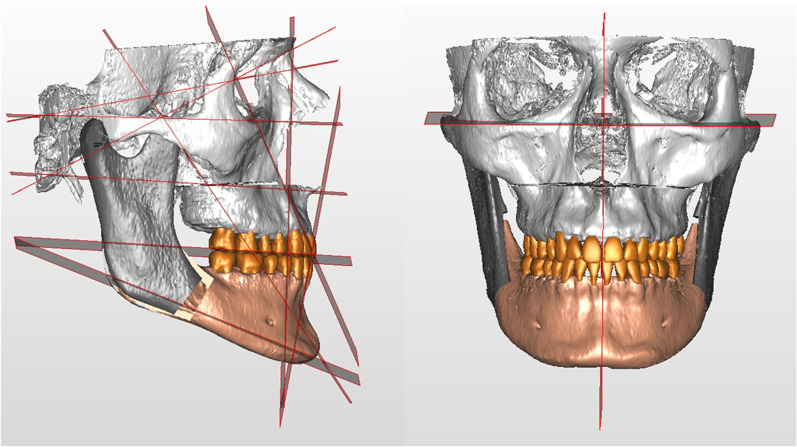
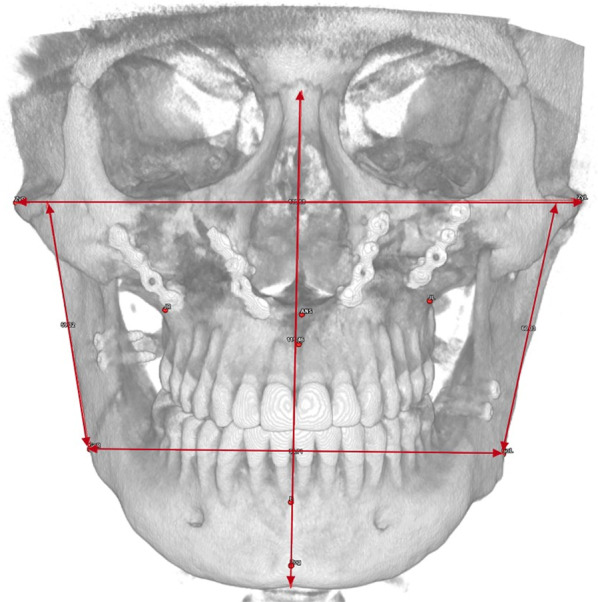
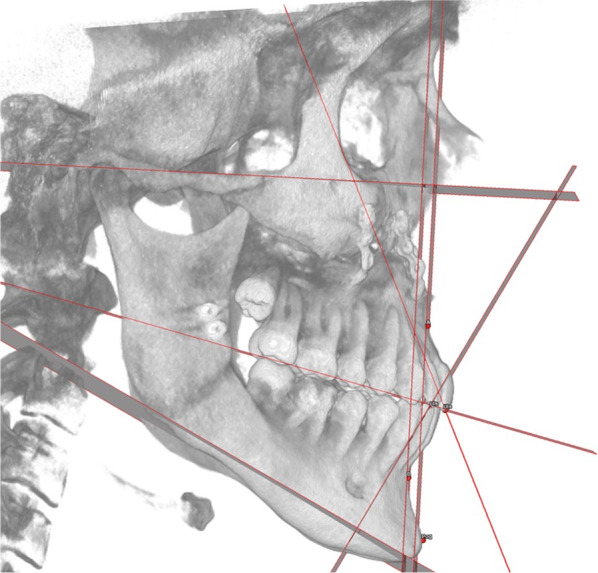
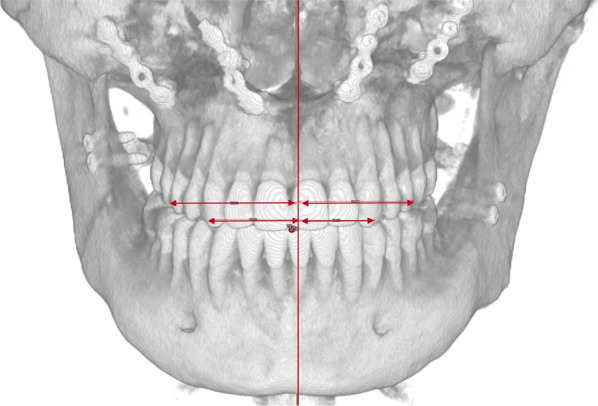
Objectives: The aim of this study is to introduce a novel 3D cephalometric analysis (3DCA) and to validate its use in evaluating the reproducibility of virtual orthodontic-surgical planning (VOSP) in surgery-first approach (SF) comparing VOSP and post-operative outcome (PostOp).
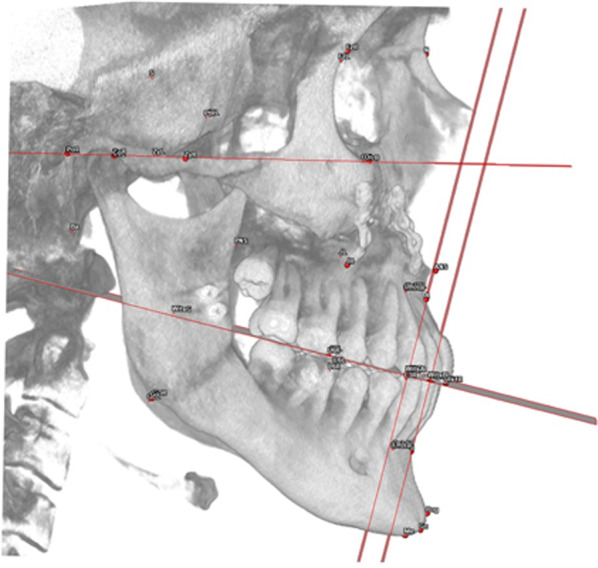
Methods: The cohort of nineteen patients underwent bimaxillary orthognathic surgery following the VOSP designed in SimPlant O&O software by processing cone-beam computed tomography (CBCT) scans and intraoral digital scanning of the dental arches. Said records were re-acquired once the post-operative orthodontic treatment was completed. The 3DCA was performed by three expert operators on VOSP and PostOp 3D models. Descriptive statistics of 3DCA measures were evaluated, and outcomes were compared via Wilcoxon test.
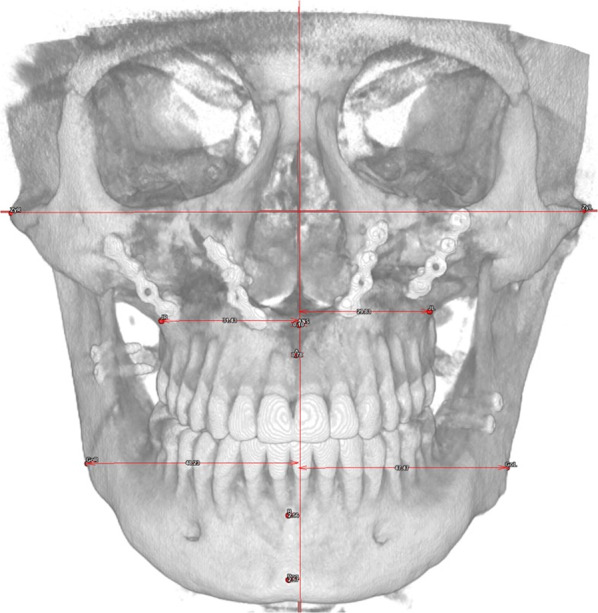
Results: In the comparison between cephalometric outcomes against planned ones, the following values showed significant differences: Wits Index, which suggests a tendency towards skeletal class III in PostOp (p = 0.033); decreased PFH/AFH ratio (p = 0.010); decreased upper incisors inclination (p < 0.001); and increased OVJ (p = 0.001). However not significant (p = 0.053), a tendency towards maxillary retroposition was found in PostOp (A/McNamara VOSP: 5.05 ± 2.64 mm; PostOp: 4.1 ± 2.6 mm). On average, however, when McNamara's plane was considered as reference, a tendency to biprotrusion was found. Upper incisal protrusion was greater in PostOp as an orthodontic compensation for residual maxillary retrusion (VOSP: 5.68 ± 2.56 mm; PostOp: 6.53 ± 2.63 mm; p = 0.084). Finally, the frontal symmetry in relation to the median sagittal plane decreased in craniocaudal direction.
Limitations: A potential limit of studies making use of closest point distance analysis is represented by the complexity that surgeons and orthodontists face in applying this three-dimensional evaluation of SF accuracy/predictability to everyday clinical practice and diagnosis. Also, heterogeneity and limited sample size may impact the results of the study comparison.
Conclusions: The presented 3DCA offers a valid aid in performing VOSP and analysing orthognathic surgery outcomes, especially in SF. Thanks to the cephalometric analysis, we found that surgery-first approach outcome unpredictability is mainly tied to the sagittal positioning of the maxilla and that the transverse symmetry is progressively less predictable in a craniocaudal direction.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures




References
-
- Yang L, Xiao Y-D, Liang Y-J, Wang X, Li J-Y, Liao G-Q. Does the surgery-first approach produce better outcomes in orthognathic surgery? a systematic review and meta-analysis. J oral Maxillofac Surg Off J Am Assoc Oral Maxillofac Surg. 2017;75(11):2422–2429. doi: 10.1016/j.joms.2017.06.002. - DOI - PubMed
-
- Janakiraman N, Feinberg M, Vishwanath M, NalakaJayaratne YS, Steinbacher DM, Nanda R, et al. Integration of 3-dimensional surgical and orthodontic technologies with orthognathic “surgery-first” approach in the management of unilateral condylar hyperplasia. Am J Orthod Dentofac Orthop. 2015;148(6):1054–1066. doi: 10.1016/j.ajodo.2015.08.012. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
