

An inflammatory state remodels the immune microenvironment and improves risk stratification in acute myeloid leukemia
- PMID: 36581735
- PMCID: PMC9986885
- DOI: 10.1038/s43018-022-00480-0
An inflammatory state remodels the immune microenvironment and improves risk stratification in acute myeloid leukemia
Erratum in
-
Author Correction: An inflammatory state remodels the immune microenvironment and improves risk stratification in acute myeloid leukemia.Nat Cancer. 2023 Jan;4(1):149. doi: 10.1038/s43018-023-00518-x. Nat Cancer. 2023. PMID: 36658429 No abstract available.
Abstract
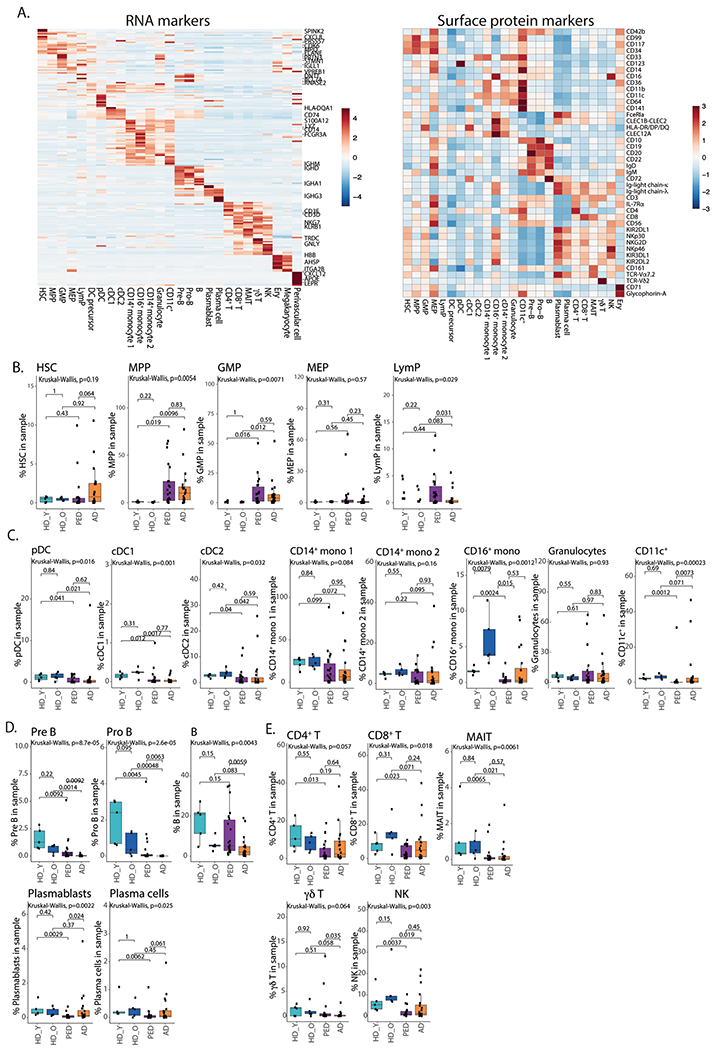
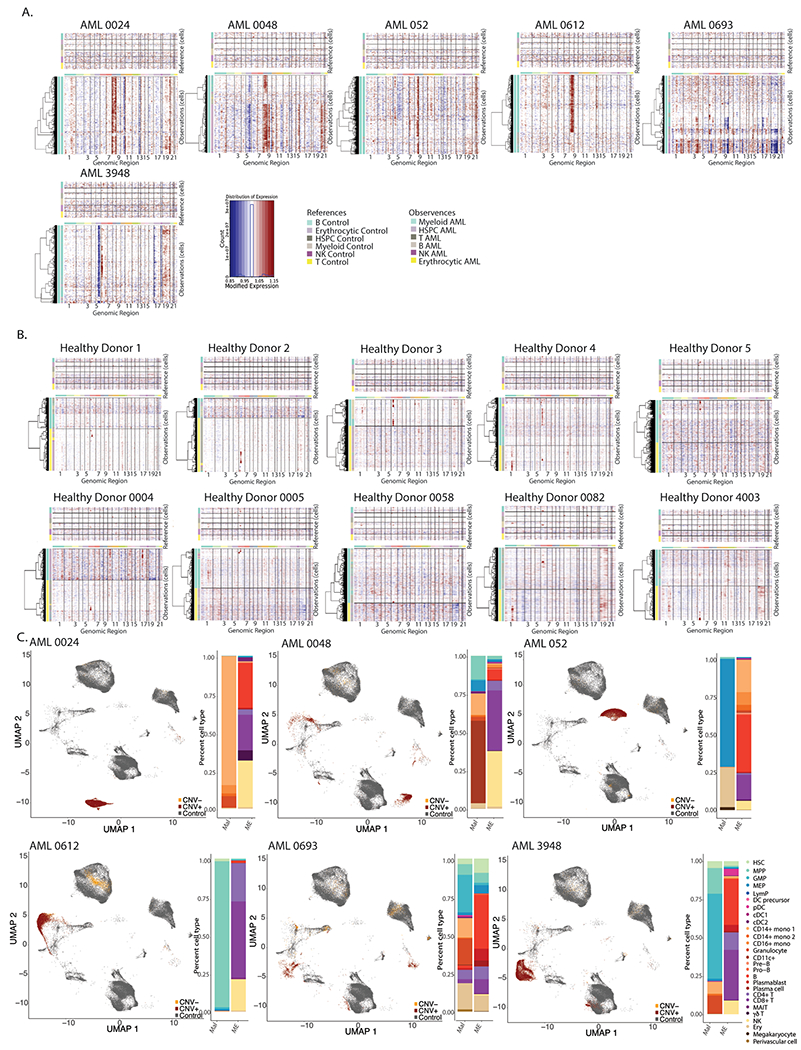
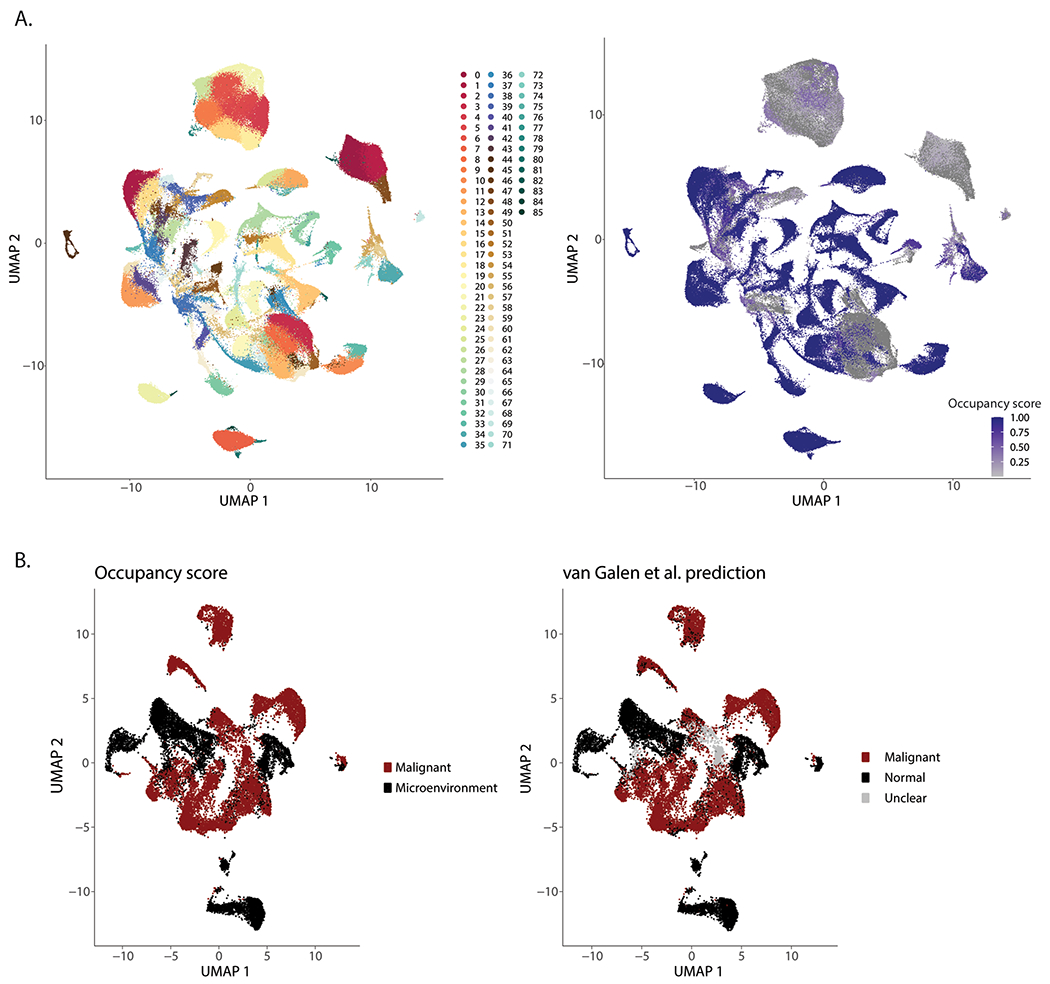
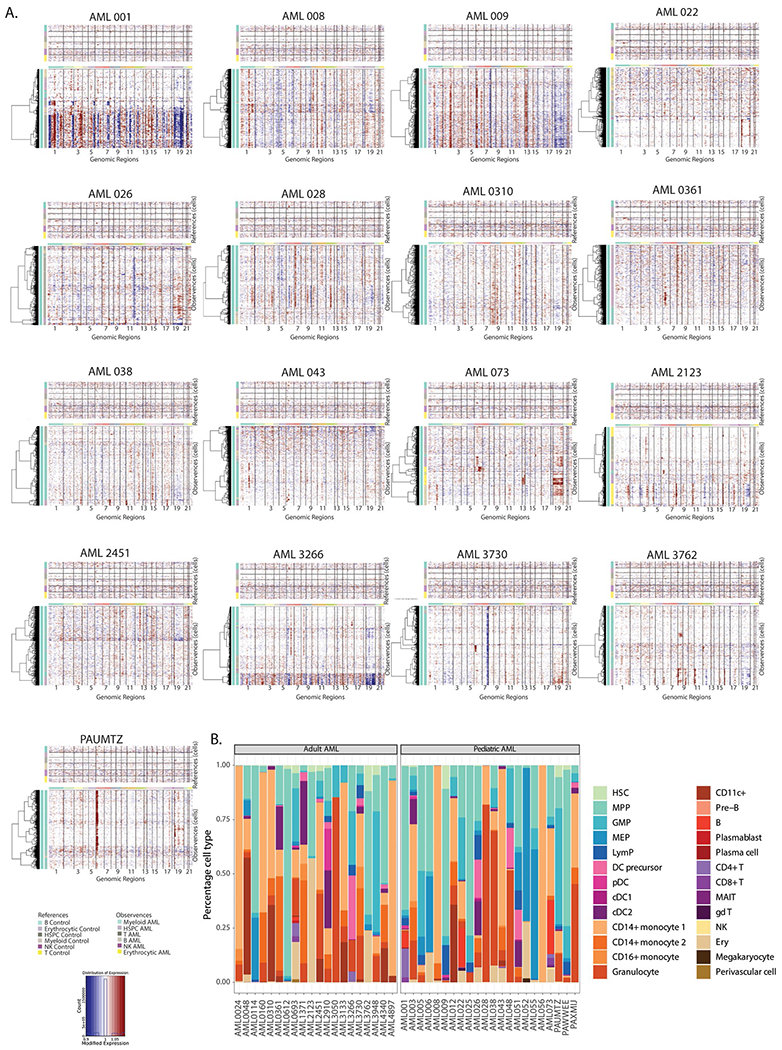
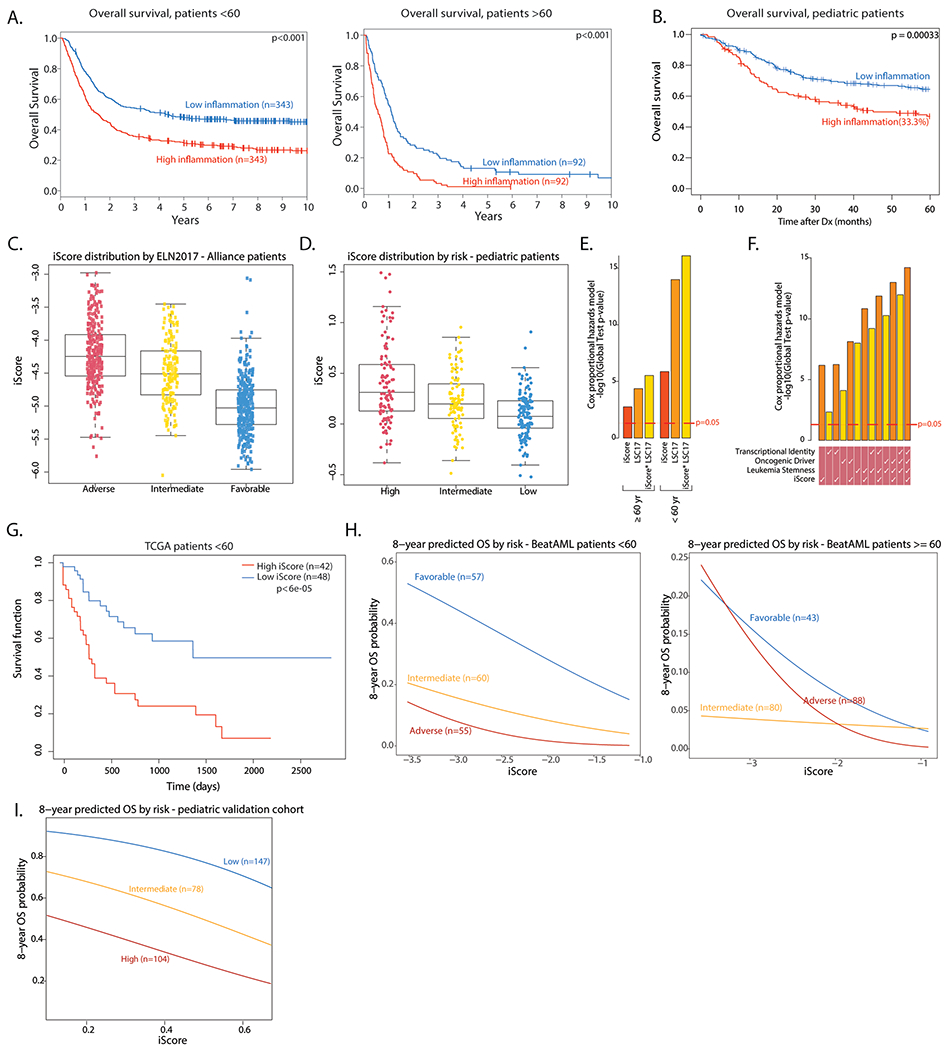
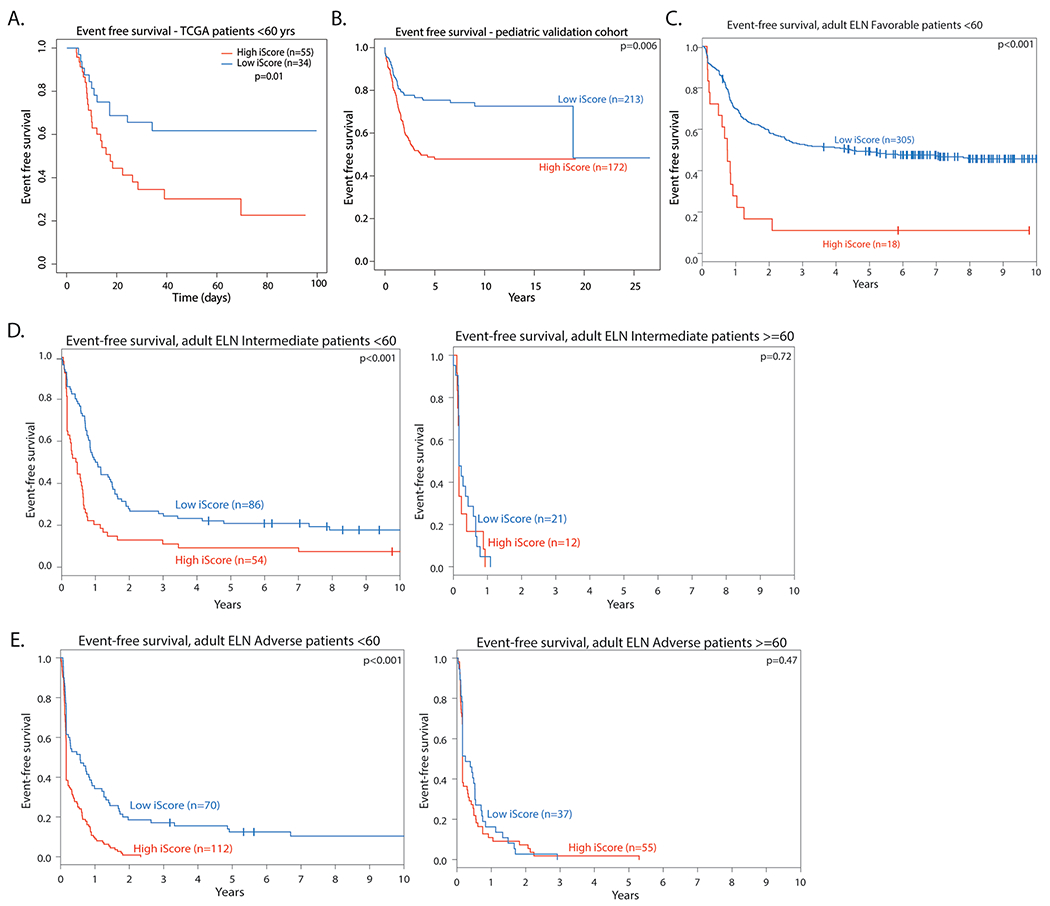
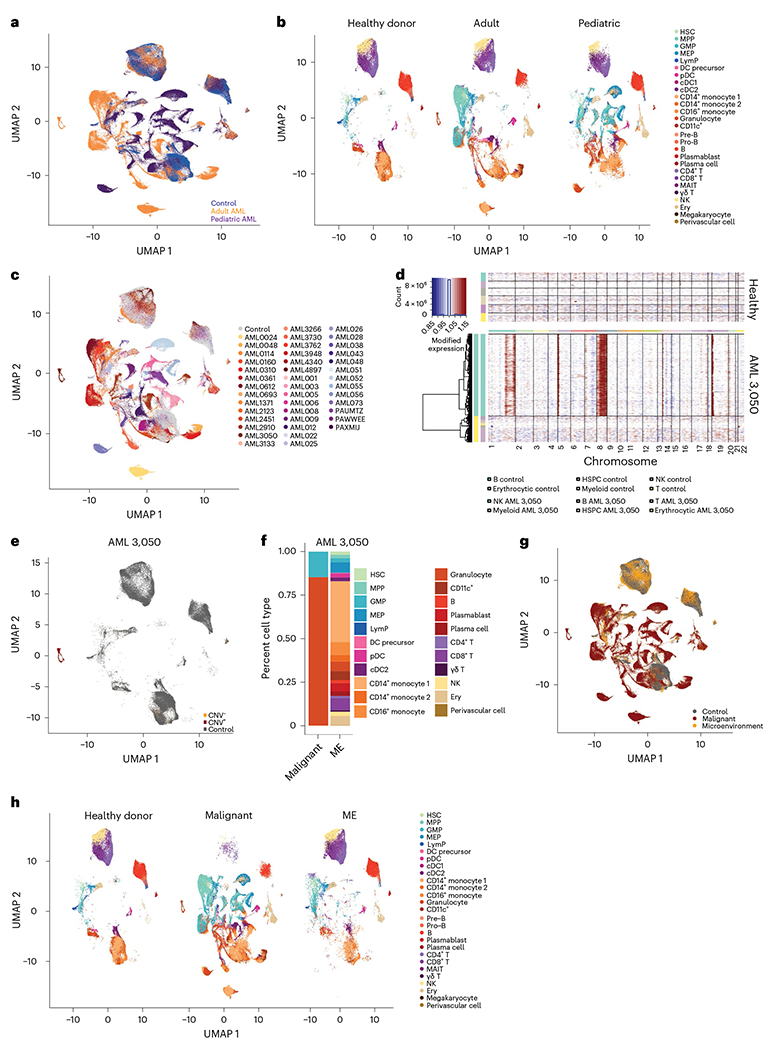
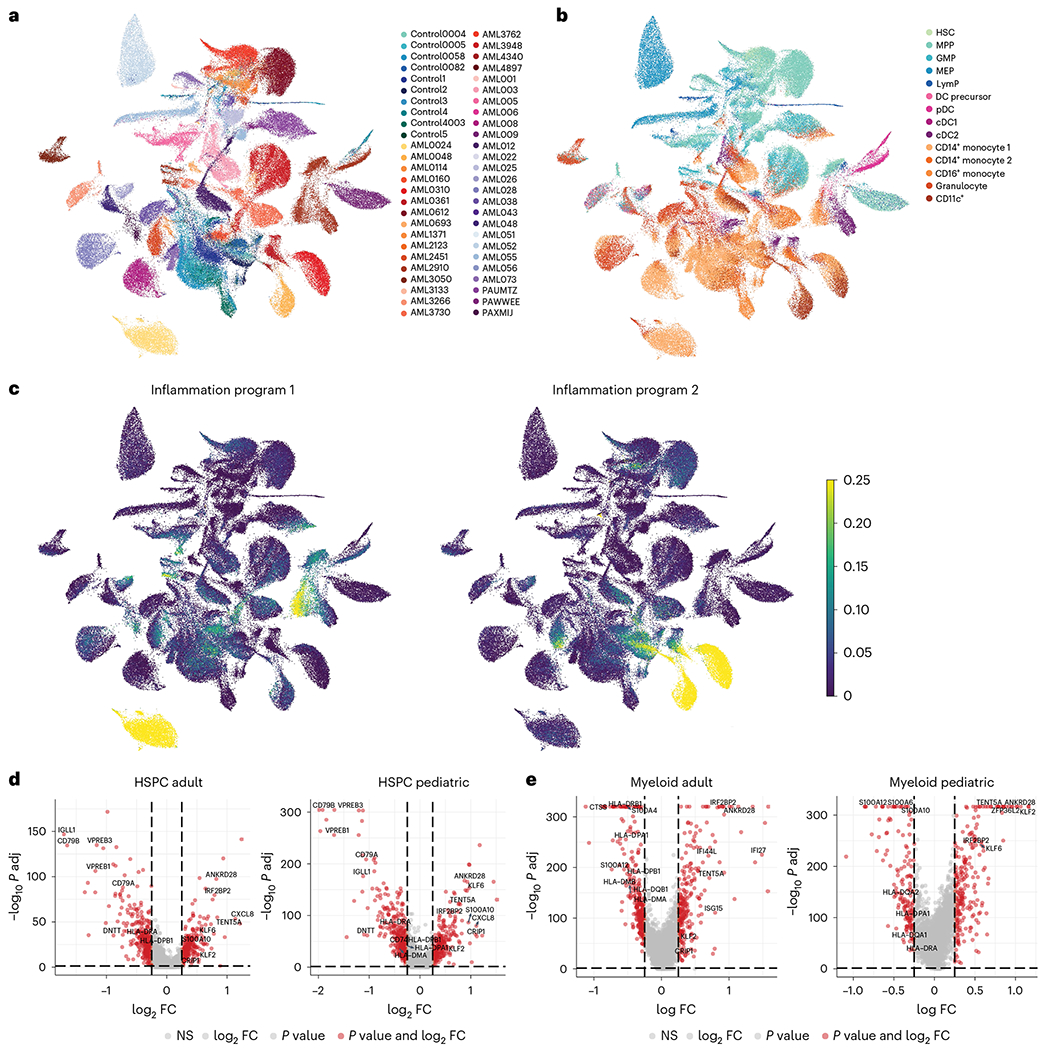
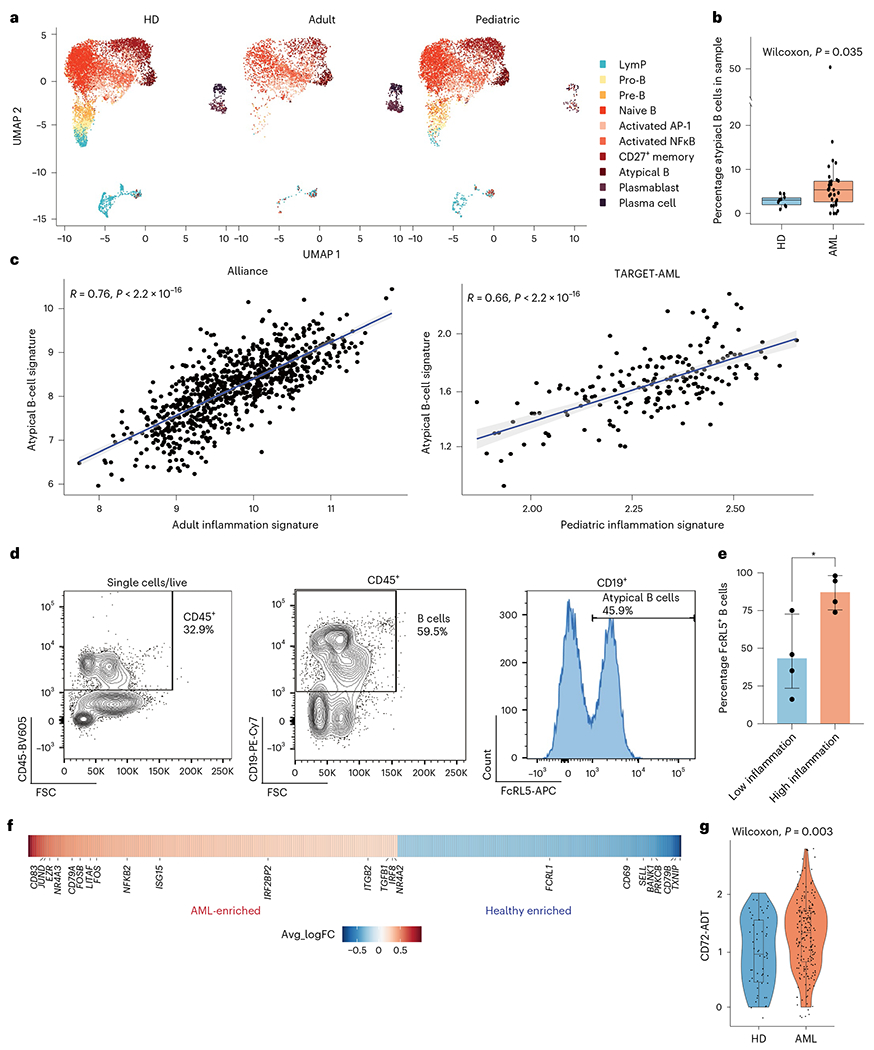
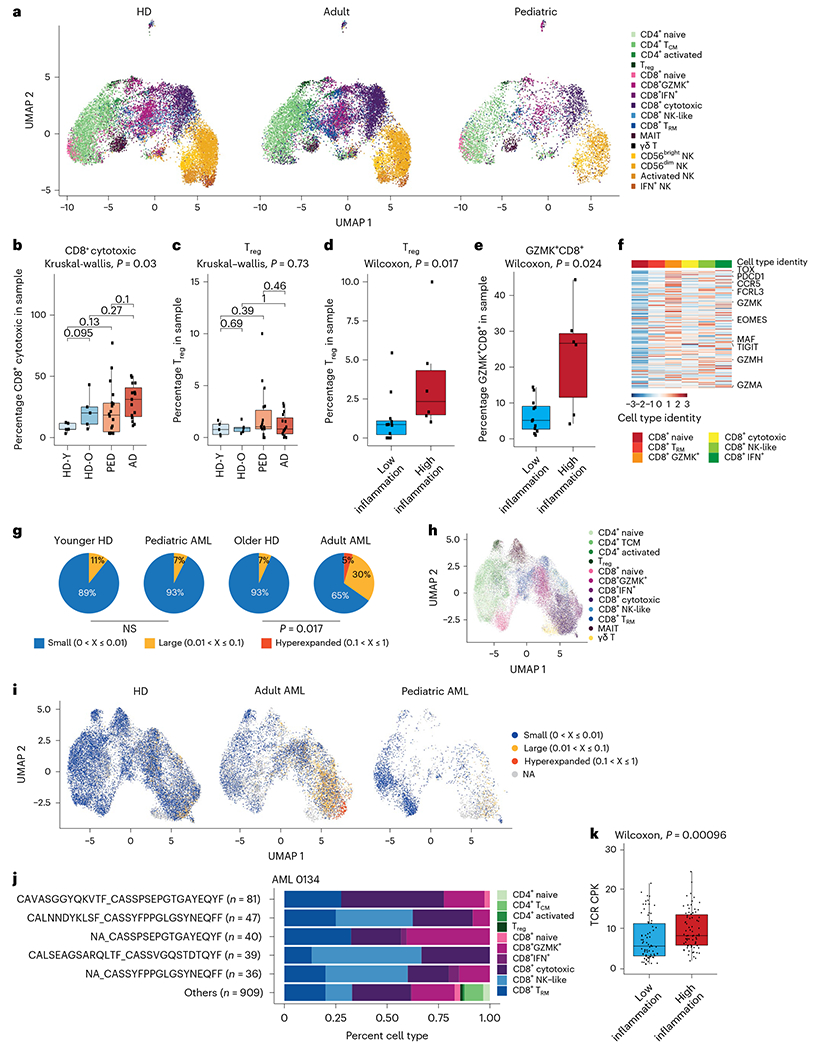
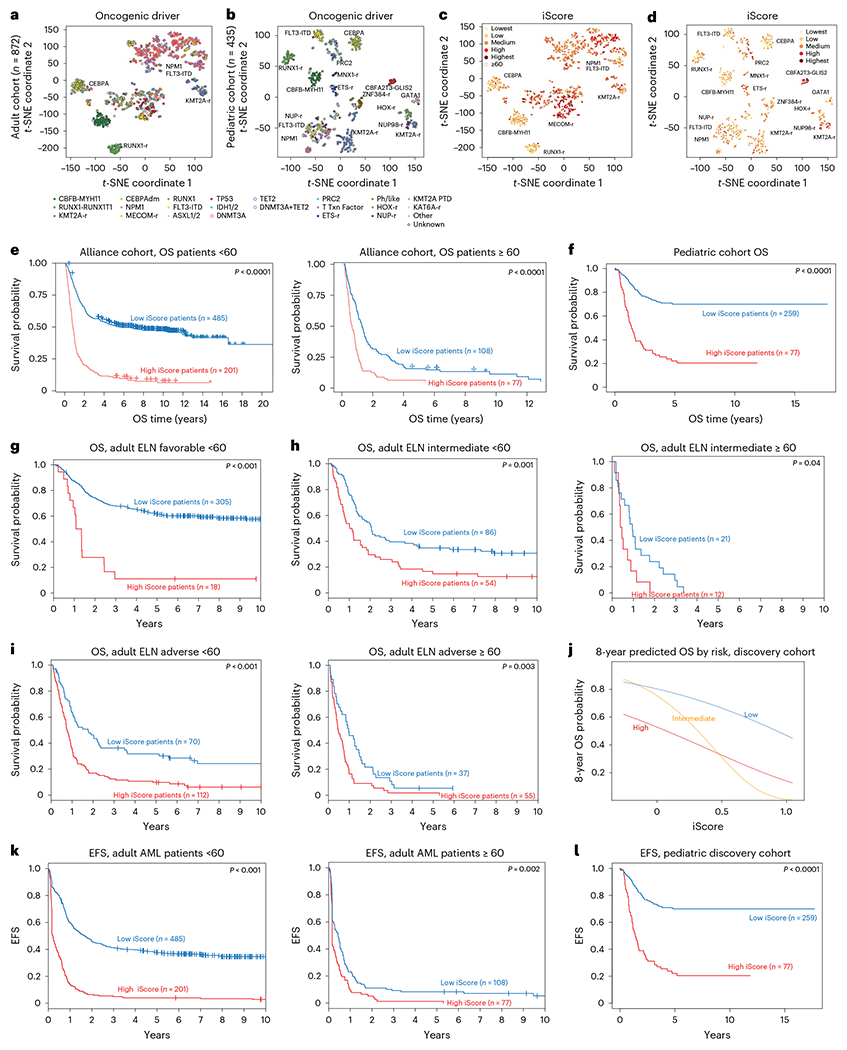
Acute myeloid leukemia (AML) is a hematopoietic malignancy with poor prognosis and limited treatment options. Here we provide a comprehensive census of the bone marrow immune microenvironment in adult and pediatric patients with AML. We characterize unique inflammation signatures in a subset of AML patients, associated with inferior outcomes. We identify atypical B cells, a dysfunctional B-cell subtype enriched in patients with high-inflammation AML, as well as an increase in CD8+GZMK+ and regulatory T cells, accompanied by a reduction in T-cell clonal expansion. We derive an inflammation-associated gene score (iScore) that associates with poor survival outcomes in patients with AML. Addition of the iScore refines current risk stratifications for patients with AML and may enable identification of patients in need of more aggressive treatment. This work provides a framework for classifying patients with AML based on their immune microenvironment and a rationale for consideration of the inflammatory state in clinical settings.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests
A.L., B.N., S.P., A.K.E., T.A.G. and A.I. submitted a patent application for the iScore patient risk stratification. I.A. is a consultant for Forsite Labs. T.A.G. is a consultant for Kura Oncology and Janssen. A.T. is a scientific advisor to Intelligencia AI.
Figures
Comment in
-
Inflammation meets translation in AML.Nat Cancer. 2023 Jan;4(1):3-4. doi: 10.1038/s43018-022-00499-3. Nat Cancer. 2023. PMID: 36721071 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
