

Implementation of a three-dimensional (3D) robotic digital microscope (AEOS) in spinal procedures
- PMID: 36581741
- PMCID: PMC9800412
- DOI: 10.1038/s41598-022-27082-1
Implementation of a three-dimensional (3D) robotic digital microscope (AEOS) in spinal procedures
Abstract
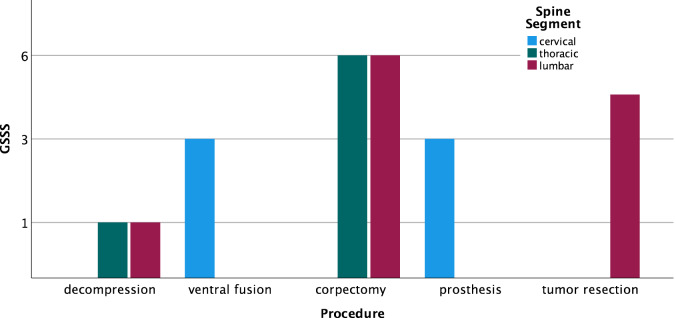
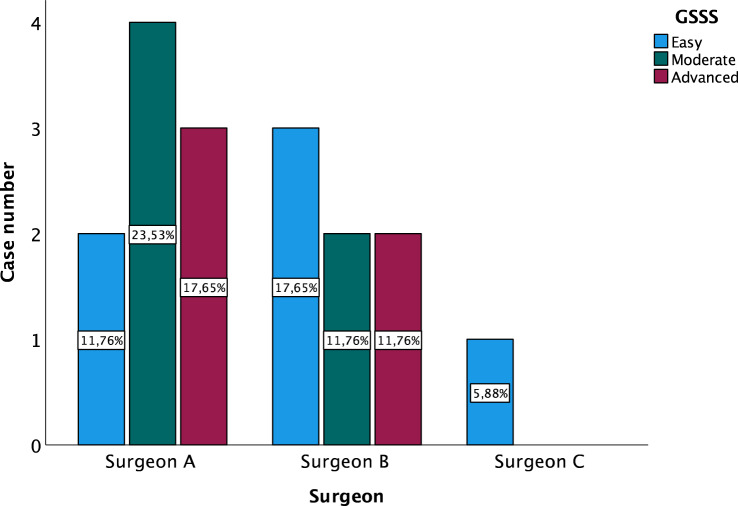
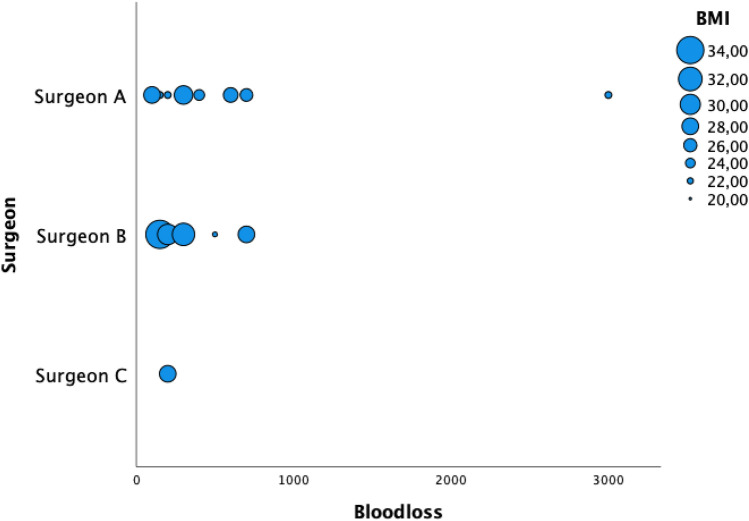
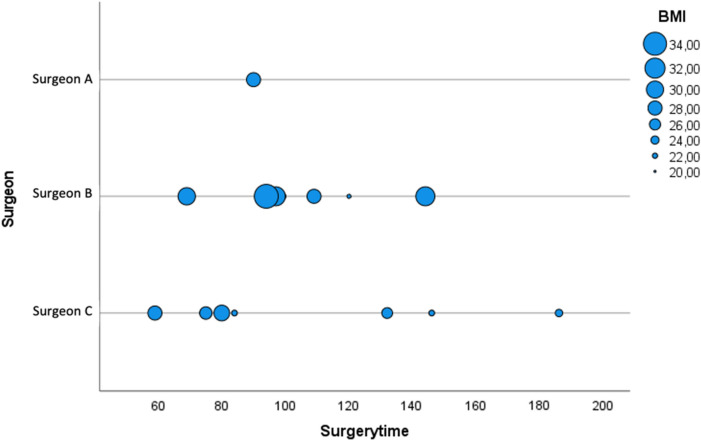
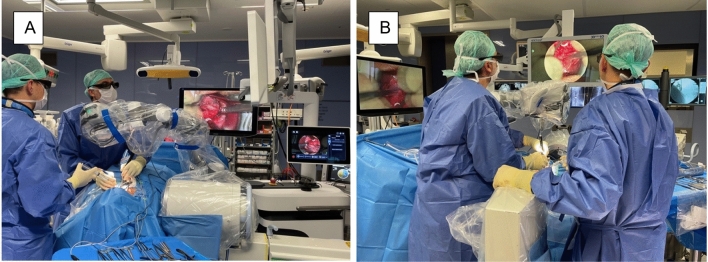
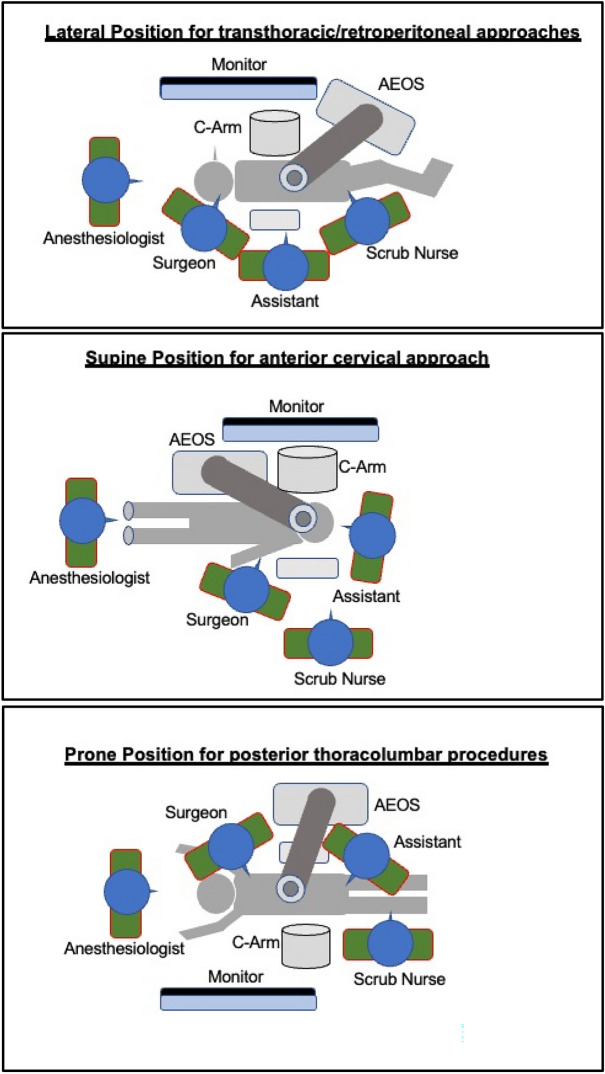
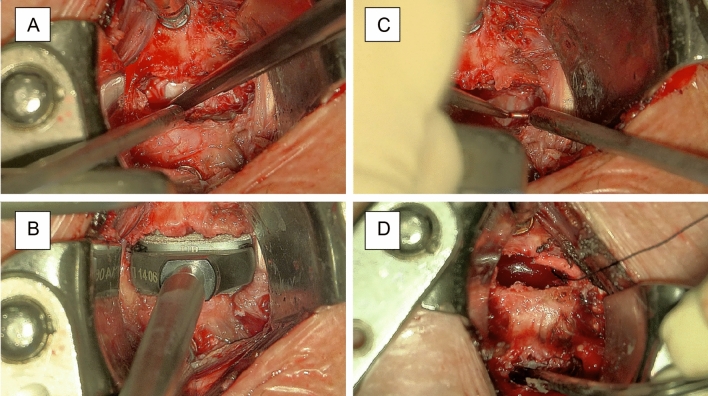
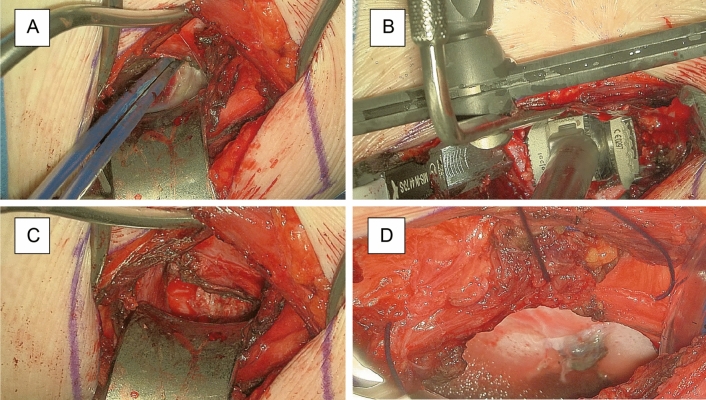
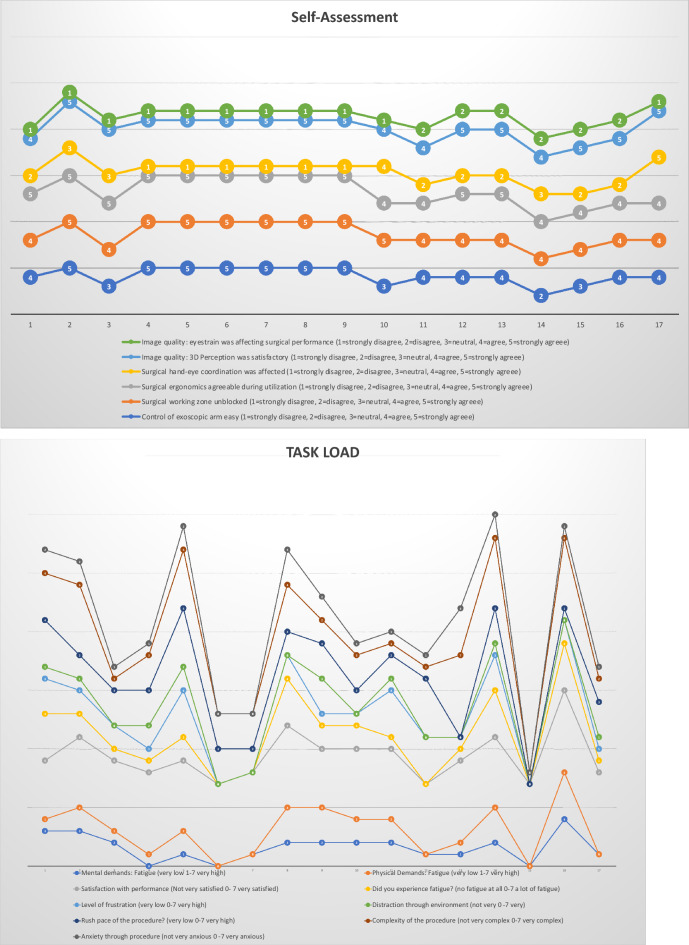
Three-dimensional exoscopes have been designed to overcome certain insufficiencies of operative microscopes. We aimed to explore the clinical use in various spinal surgeries. We performed surgery on patients with different spine entities in a neurosurgical department according to the current standard operating procedures over a 4-week period of time. The microsurgical part has been performed with Aesculap AEOS 3D microscope. Three neurosurgeons with different degree of surgical expertise completed a questionnaire with 43 items based on intraoperative handling and feasibility after the procedures. We collected and analyzed data from seventeen patients (35% male/65% female) with a median age of 70 years [CI 47-86] and median BMI of 25.8 kg/m2 [range 21-33]. We included a variety of spinal pathologies (10 degenerative, 4 tumor and 3 infectious cases) with different level of complexity. Regarding setup conflicts we observed issues with adjustment of the monitor position or while using additional equipment (e.g. fluoroscopy in fusion surgery) (p = 0.007/p = 0.001). However image resolution and sharpness as well as 3D-depth perception were completely satisfactory for all surgeons in all procedures. The utilization of the exoscopic arm was easy for 76.5% of the surgeons, and all of them declared a significant improvement of the surgical corridor. The 3D-exoscope implementation appears to achieve very satisfactory results in spinal procedures especially with minimally invasive approaches.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
