

What is the agreement between intraoperative fluoroscopy and postoperative radiographs in Bernese periacetabular osteotomy?
- PMID: 36581915
- PMCID: PMC9801538
- DOI: 10.1186/s12891-022-06054-6
What is the agreement between intraoperative fluoroscopy and postoperative radiographs in Bernese periacetabular osteotomy?
Abstract
Background: It is important to reorient the acetabular fragment into an optimal position and version to ensure a good long-term outcome after Bernese periacetabular osteotomy (PAO). Unfortunately, the intraoperative balance between overcorrection and undercorrection remains challenging for the surgeon. The purpose of this study was to answer two questions: (1) Does the femoral head coverage measured on intraoperative fluoroscopy agree with that measured on postoperative radiography? (2) What is the reliability of intraoperative fluoroscopy in identifying hip center correction in PAO?
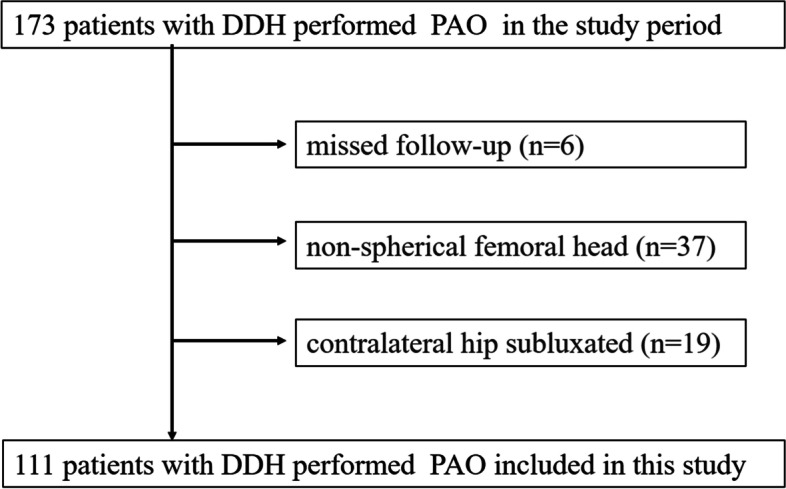
Methods: A total of 173 patients (173 hips) who underwent PAO for developmental dysplasia of the hip (DDH) at our center from July 01, 2020, to December 31, 2020, were retrospectively reviewed. Imaging data from 111 patients (female/male, 98/13; right/left, 72/39; mean age, 28.93 years) were included in this study. The analysis included measurement of the lateral center-edge angle (LCEA), acetabular index (AI), anterior wall index (AWI), posterior wall index (PWI), extrusion index (EI), and medial offset distance (MO). These measurements were acquired from intraoperative fluoroscopic images and postoperative radiographs and compared by paired t test using SPSS (version 24.0). Significance was determined at a p value of < 0.05. Bland-Altman analysis, conducted using GraphPad Software (version 9), was used to quantify the agreement between intraoperative fluoroscopic images and postoperative radiographs.
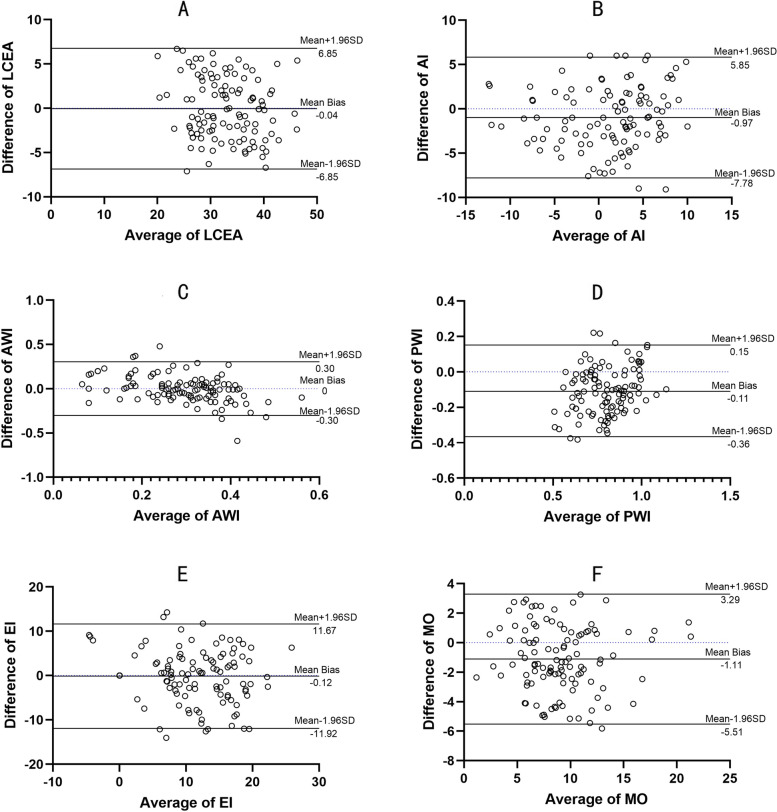
Results: The means (standard deviations, SDs) of the LCEA, AI, AWI, PWI, EI, and MO obtained on intraoperative fluoroscopy were 32.86° (5.73°), 0.66° (5.55), 0.29 (0.10), 0.75 (0.17), 11.15% (6.50%), and 8.49 mm (3.68 mm), respectively. On postoperative radiography, the corresponding values were 32.91° (6.31°), 1.63° (5.22°), 0.29 (0.15), 0.85 (0.14), 11.27% (7.36%), and 9.60 mm (3.79 mm). The differences in the LCEA, AWI, and EI acquired from intraoperative fluoroscopic images and postoperative radiographs were not significant (p = 0.90, 0.95, and 0.83, respectively), but those in the AI, PWI, and MO were significant (p < 0.05). The mean biases (95% limits of agreement) of the LCEA, AI, AWI, PWI, EI, and MO were - 0.04 (- 6.85), - 0.97 (- 7.78), 0 (- 0.30), - 0.11 (- 0.36), - 0.12 (- 11.92), and - 1.11 (- 5.51), respectively.
Conclusion: The LCEA, EI, and AWI can be used to reliably predict postoperative femoral head coverage at the level of 2D graphics. Acetabular inclination can be cautiously assessed using AI on intraoperative fluoroscopy. In the absence of intraoperative 3D image evaluation, the AWI and PWI demonstrate acceptable agreement between fluoroscopy and radiography in assessing the acetabular version. Although the MO shows slight bias, it can be helpful in properly positioning the acetabulum during PAO.
Keywords: Agreement; Hip parameters; Intraoperative fluoroscopy; Periacetabular osteotomy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
What Is the Reliability and Accuracy of Intraoperative Fluoroscopy in Evaluating Anterior, Lateral, and Posterior Coverage During Periacetabular Osteotomy?Clin Orthop Relat Res. 2019 May;477(5):1138-1144. doi: 10.1097/CORR.0000000000000616. Clin Orthop Relat Res. 2019. PMID: 30676406 Free PMC article.
-
Do Radiographic Parameters of Dysplasia Improve to Normal Ranges After Bernese Periacetabular Osteotomy?Clin Orthop Relat Res. 2017 Apr;475(4):1120-1127. doi: 10.1007/s11999-016-5077-8. Clin Orthop Relat Res. 2017. PMID: 27646418 Free PMC article.
-
Medialization of the Hip's Center with Periacetabular Osteotomy: Validation of Assessment with Plain Radiographs.Clin Orthop Relat Res. 2021 May 1;479(5):1040-1049. doi: 10.1097/CORR.0000000000001572. Clin Orthop Relat Res. 2021. PMID: 33861214 Free PMC article.
-
Periacetabular osteotomy in the treatment of severe acetabular dysplasia. Surgical technique.J Bone Joint Surg Am. 2006 Mar;88 Suppl 1 Pt 1:65-83. doi: 10.2106/JBJS.E.00887. J Bone Joint Surg Am. 2006. PMID: 16510801 Review.
-
Bernese periacetabular osteotomy (PAO): from its local inception to its worldwide adoption.J Orthop Traumatol. 2023 Nov 2;24(1):55. doi: 10.1186/s10195-023-00734-2. J Orthop Traumatol. 2023. PMID: 37917385 Free PMC article. Review.
Cited by
-
Medial meniscus tears are most prevalent in type I ACL tears, while type I ACL tears only account for 8% of all ACL tears.Knee Surg Sports Traumatol Arthrosc. 2023 Jun;31(6):2349-2357. doi: 10.1007/s00167-022-07068-2. Epub 2022 Jul 17. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 35842857
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
