

Left versus right approach for middle and lower esophageal squamous cell carcinoma: A propensity score-matched study
- PMID: 36582805
- PMCID: PMC9792602
- DOI: 10.3389/fonc.2022.858660
Left versus right approach for middle and lower esophageal squamous cell carcinoma: A propensity score-matched study
Abstract
Background: Despite superior short-term outcomes, there is considerable debate about the oncological efficacy of the left approach esophagectomy for middle and lower squamous esophageal carcinoma (ESCC). A propensity score-matched retrospective study was conducted to evaluate the left approach's short- and long-term effects.
Methods: We recorded data from patients with ESCC who underwent curative resection via the left or right approach between January 2010 and December 2015. Propensity score matching (PSM) was performed, and maximally selected rank statistics (MSRS) were utilized to determine the appropriate number of lymph nodes to resect during esophagectomy.
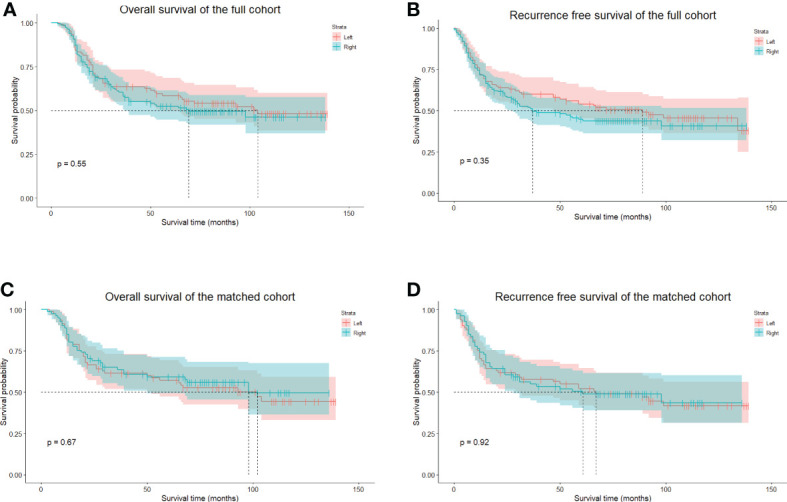
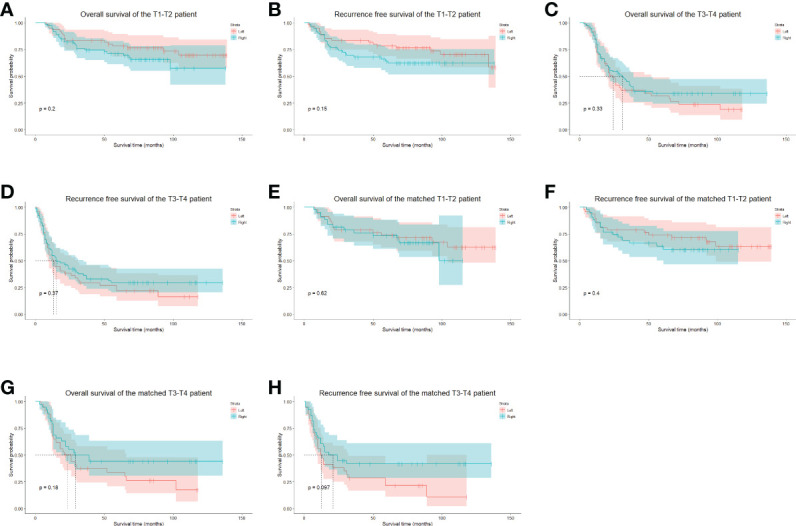
Results: One hundred and forty-eight ESCC patients underwent esophagectomy via the right approach, and 108 underwent the left approach esophagectomy. After PSM, the left approach esophagectomy showed statistically significant superiority in operative time and time to oral intake, and there was a trend toward a shorter length of hospital stay. Fewer cervical, upper thoracic, and recurrent laryngeal nerve lymph nodes were harvested via the left approach than the right approach; the total number of lymph nodes harvested via the left and right approaches was similar. Similar long-term survival outcomes were achieved. MSRS suggested that at least 25 lymph nodes are needed to be resected during esophagectomy to improve survival in N0 patients.
Conclusions: The left approach esophagectomy might facilitate postoperative recovery in patients with middle and lower ESCC. With adequate lymphadenectomy, the left approach esophagectomy might achieve similar long-term outcomes for middle and lower ESCC patients.
Keywords: Ivor-Lewis procedure; McKeown procedure; Sweet procedure; esophageal squamous cell carcinoma; lymphadenectomy.
Copyright © 2022 Zhang, Qi, Huang, Liu, Lin and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous