

A randomized phase 2 study of neoadjuvant carboplatin and paclitaxel with or without atezolizumab in triple negative breast cancer (TNBC) - NCI 10013
- PMID: 36585404
- PMCID: PMC9803651
- DOI: 10.1038/s41523-022-00500-3
A randomized phase 2 study of neoadjuvant carboplatin and paclitaxel with or without atezolizumab in triple negative breast cancer (TNBC) - NCI 10013
Abstract
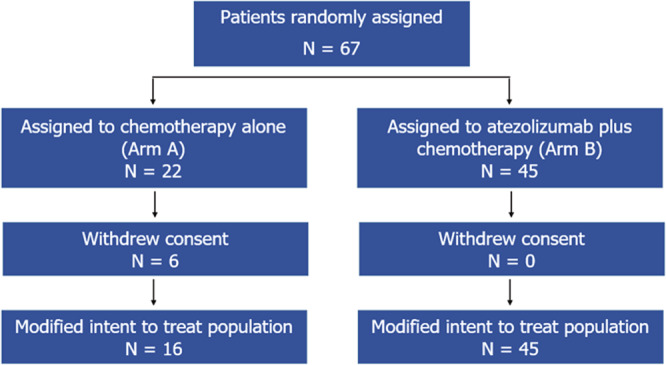
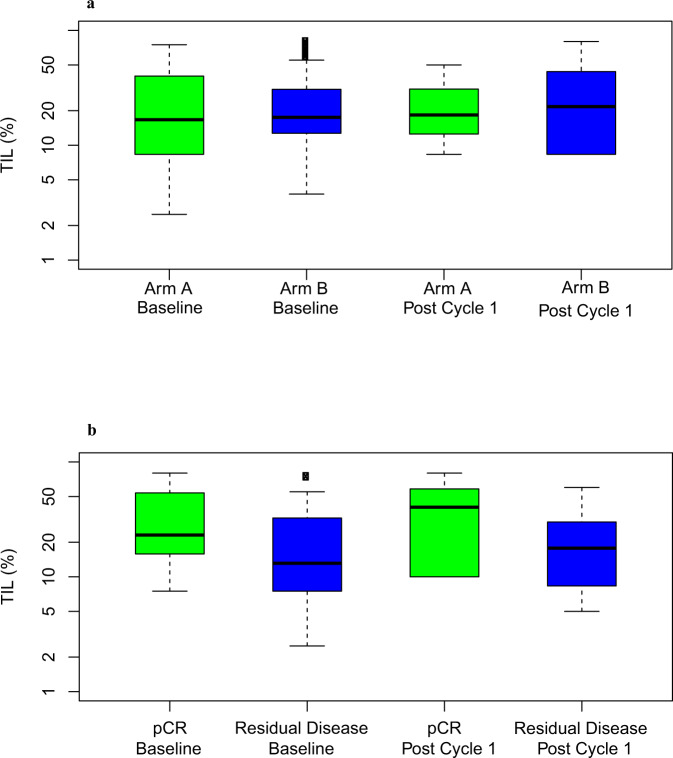
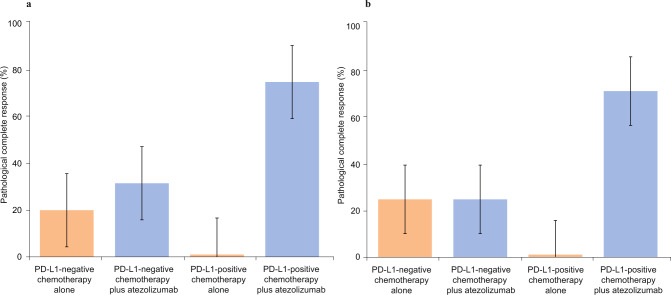
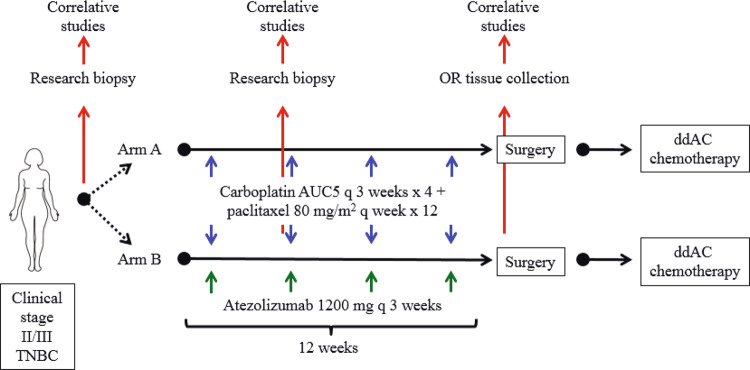
Atezolizumab with chemotherapy has shown improved progression-free and overall survival in patients with metastatic PD-L1 positive triple negative breast cancer (TNBC). Atezolizumab with anthracycline- and taxane-based neoadjuvant chemotherapy has also shown increased pathological complete response (pCR) rates in early TNBC. This trial evaluated neoadjuvant carboplatin and paclitaxel with or without atezolizumab in patients with clinical stages II-III TNBC. The co-primary objectives were to evaluate if chemotherapy and atezolizumab increase pCR rate and tumor infiltrating lymphocyte (TIL) percentage compared to chemotherapy alone in the mITT population. Sixty-seven patients (ages 25-78 years; median, 52 years) were randomly assigned - 22 patients to Arm A, and 45 to Arm B. Median follow up was 6.6 months. In the modified intent to treat population (all patients evaluable for the primary endpoints who received at least one dose of combination therapy), the pCR rate was 18.8% (95% CI 4.0-45.6%) in Arm A, and 55.6% (95% CI 40.0-70.4%) in Arm B (estimated treatment difference: 36.8%, 95% CI 8.5-56.6%; p = 0.018). Grade 3 or higher treatment-related adverse events occurred in 62.5% of patients in Arm A, and 57.8% of patients in Arm B. One patient in Arm B died from recurrent disease during the follow-up period. TIL percentage increased slightly from baseline to cycle 1 in both Arm A (mean ± SD: 0.6% ± 21.0%) and Arm B (5.7% ± 15.8%) (p = 0.36). Patients with pCR had higher median TIL percentages (24.8%) than those with non-pCR (14.2%) (p = 0.02). Although subgroup analyses were limited by the small sample size, PD-L1-positive patients treated with chemotherapy and atezolizumab had a pCR rate of 75% (12/16). The addition of atezolizumab to neoadjuvant carboplatin and paclitaxel resulted in a statistically significant and clinically relevant increased pCR rate in patients with clinical stages II and III TNBC. (Funded by National Cancer Institute).
© 2022. The Author(s).
Conflict of interest statement
F.O.A. declares no competing non-financial interests but the following competing financial interests from Astra Zeneca, Gilead, Biotheranostics, Athenex, QED, Cardinal Health, Teladoc Health, Pfizer, and research grants to her institution from Pfizer, Seattle Genetics, Immunomedics, NeoImmuneTech, RNA Diagnostics, Astellas. F.G., C.R.S., I.C. and D.W.N. declare no competing financial or non-financial interests. R.W. declares competing financial interests from Seagen and declares competing non-financial interests as a scientific steering committee member for Celcuity. M.A. declares no competing financial or non-financial interests. A.B. declares no competing non-financial interests but the following competing financial interests from Roche, Pfizer, Astra Zeneca, and Merck. C.D. declares no competing financial or non-financial interests. C.A.S.-M. declares no competing non-financial interests but the following competing financial interests from Seattle Genetics, Genomic Health, Athenex, Polyphor, Halozyme, and research grants to his institution from Astrazeneca, Pfizer, Novartis, Tesaro/GSK. R.M.C. declares no competing non-financial interests but the following competing financial interests as research grants to her institution from Novartis, Puma Biotechnology, Merck, Genentech, and Macrogenics. J.F. declares no competing non-financial interests but the following competing financial interests from Genomic Health, and ownership interests in Genomic Health, and Immunomedics. A.M.-A. declares no competing non-financial interests but the following competing financial interests as research grants to his institution from Genentech, GSK. J.M.H., M.C., S.R.D., S.L., K.L.P., S.M.J., J.L.W., A.G.-H., S.J.R., Z.L., I.H., E.S. and W.E.G. declare no competing financial or non-financial interests.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
