

Association of Phenotypic Aging Marker with comorbidities, frailty and inflammatory markers in people living with HIV
- PMID: 36585655
- PMCID: PMC9805022
- DOI: 10.1186/s12877-022-03720-1
Association of Phenotypic Aging Marker with comorbidities, frailty and inflammatory markers in people living with HIV
Abstract
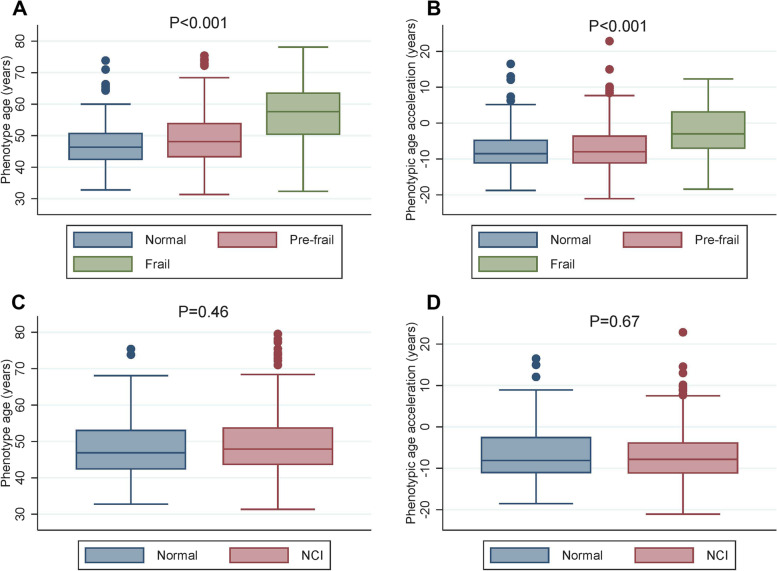
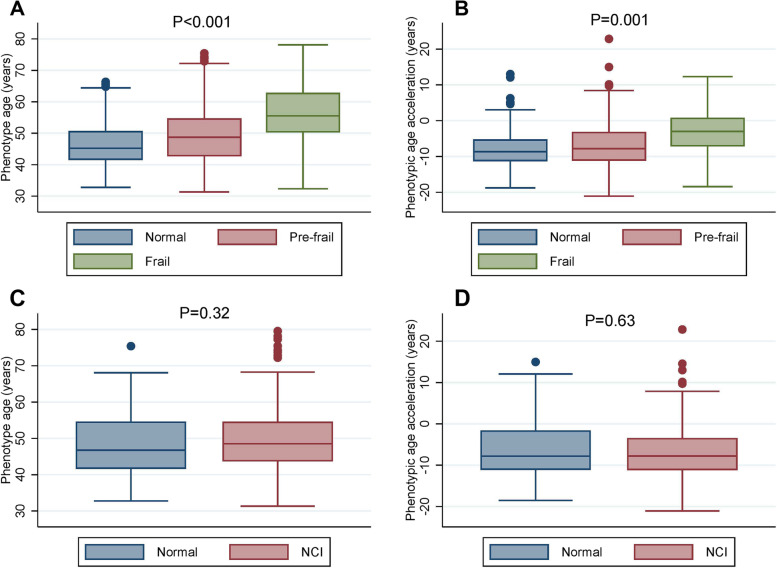
Background: Aging characteristics in people living with HIV (PLWH) are heterogeneous, and the identification of risk factors associated with aging-related comorbidities such as neurocognitive impairment (NCI) and frailty is important. We evaluated predictors of novel aging markers, phenotypic age (PhenoAge) and phenotypic age acceleration (PAA) and their association with comorbidities, frailty, and NCI.
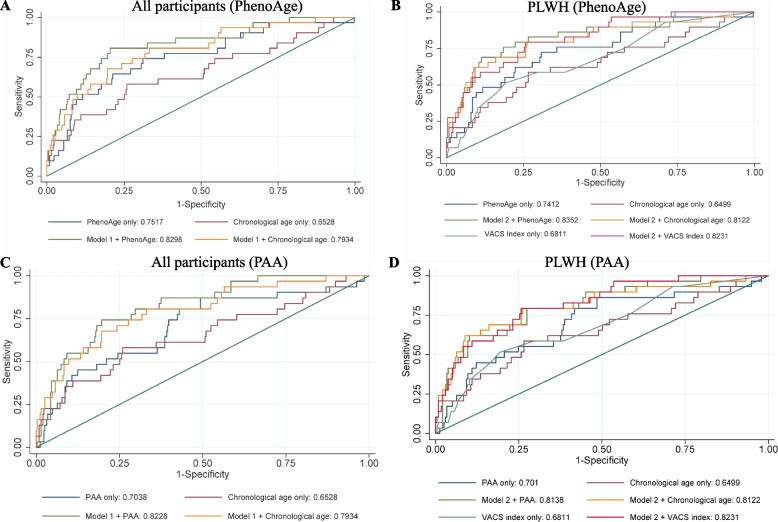
Methods: In a cohort of PLWH and age- and sex-matched HIV-negative controls, we calculated PhenoAge using chronological age and 9 biomarkers from complete blood counts, inflammatory, metabolic-, liver- and kidney-related parameters. PAA was calculated as the difference between chronological age and PhenoAge. Multivariate logistic regression models were used to identify the factors associated with higher (>median) PAA. Area under the receiver operating characteristics curve (AUROC) was used to assess model discrimination for frailty.
Results: Among 333 PLWH and 102 HIV-negative controls (38% female), the median phenotypic age (49.4 vs. 48.5 years, p = 0.54) and PAA (- 6.7 vs. -7.5, p = 0.24) was slightly higher and PAA slightly less in PLWH although this did not reach statistical significance. In multivariate analysis, male sex (adjusted odds ratio = 1.68 [95%CI = 1.03-2.73]), current smoking (2.74 [1.30-5.79]), diabetes mellitus (2.97 [1.48-5.99]), hypertension (1.67 [1.02-2.72]), frailty (3.82 [1.33-10.93]), and higher IL-6 levels (1.09 [1.04-1.15]), but not HIV status and NCI, were independently associated with higher PAA. PhenoAge marker discriminated frailty better than chronological age alone (AUROC: 0.75 [0.66-0.85] vs. 0.65 [0.55-0.77], p = 0.04). In the analysis restricted to PLWH, PhenoAge alone predicted frailty better than chronological age alone (AUROC: 0.7412 vs. 0.6499, P = 0.09) and VACS index (AUROC: 0.7412 vs. 0.6811, P = 0.34) despite not statistically significant.
Conclusions: While PLWH did not appear to have accelerated aging in our cohort, the phenotypic aging marker was significantly associated with systemic inflammation, frailty, and cardiovascular disease risk factors. This simple aging marker could be useful to identify high-risk PLWH within a similar chronological age group.
Keywords: Aging; Comorbidities; Frailty; HIV/AIDS; Phenotypic age acceleration; Phenotypic aging marker; Thailand.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Alcohol use, physical activity, and muscle strength moderate the relationship between body composition and frailty risk among people living with HIV.Alcohol Clin Exp Res. 2022 Nov;46(11):2041-2053. doi: 10.1111/acer.14941. Epub 2022 Oct 20. Alcohol Clin Exp Res. 2022. PMID: 36124866 Free PMC article.
-
Frailty, Neurocognitive Impairment, or Both in Predicting Poor Health Outcomes Among Adults Living With Human Immunodeficiency Virus.Clin Infect Dis. 2019 Jan 1;68(1):131-138. doi: 10.1093/cid/ciy430. Clin Infect Dis. 2019. PMID: 29788039 Free PMC article.
-
Associations of combined phenotypic aging and genetic risk with incident cancer: A prospective cohort study.Elife. 2024 Apr 30;13:RP91101. doi: 10.7554/eLife.91101. Elife. 2024. PMID: 38687190 Free PMC article.
-
Frailty in older people living with HIV: current status and clinical management.BMC Geriatr. 2022 Nov 30;22(1):919. doi: 10.1186/s12877-022-03477-7. BMC Geriatr. 2022. PMID: 36447144 Free PMC article. Review.
-
Frailty and prefrailty in people living with HIV, with focus on women living with HIV.Int J STD AIDS. 2022 Nov;33(13):1106-1110. doi: 10.1177/09564624221127744. Epub 2022 Oct 11. Int J STD AIDS. 2022. PMID: 36217985 Review.
Cited by
-
Association of Physical Activity with Phenotypic Age among Populations with Different Breakfast Habits.Nutrients. 2024 Feb 20;16(5):575. doi: 10.3390/nu16050575. Nutrients. 2024. PMID: 38474704 Free PMC article.
-
Better Life's Essential 8 contributes to slowing the biological aging process: a cross-sectional study based on NHANES 2007-2010 data.Front Public Health. 2024 Mar 13;12:1295477. doi: 10.3389/fpubh.2024.1295477. eCollection 2024. Front Public Health. 2024. PMID: 38544722 Free PMC article.
-
Association of biological aging with frailty and post-transplant outcomes among adults with cirrhosis.Geroscience. 2024 Jun;46(3):3287-3295. doi: 10.1007/s11357-024-01076-5. Epub 2024 Jan 21. Geroscience. 2024. PMID: 38246968 Free PMC article.
-
Age-related clonal hematopoiesis and HIV infection are associated with geriatric outcomes: The ARCHIVE study.Cell Rep Med. 2024 Dec 17;5(12):101835. doi: 10.1016/j.xcrm.2024.101835. Epub 2024 Dec 2. Cell Rep Med. 2024. PMID: 39626674 Free PMC article.
-
Forecasting and validating fat mass ratio models through anthropometric measurements and health-related factors among people with HIV: a cross-sectional investigation.Ann Transl Med. 2024 Jun 10;12(3):44. doi: 10.21037/atm-23-1946. Epub 2024 May 29. Ann Transl Med. 2024. PMID: 38911564 Free PMC article.
References
-
- Schouten J, Wit FW, Stolte IG, Kootstra NA, van der Valk M, Geerlings SE, et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clin Infect Dis. 2014;59(12):1787–1797. doi: 10.1093/cid/ciu701. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
