

Predictors of bleeding events in acute decompensated heart failure patients with antithrombotic therapy: AURORA study
- PMID: 36585753
- PMCID: PMC10053354
- DOI: 10.1002/ehf2.14277
Predictors of bleeding events in acute decompensated heart failure patients with antithrombotic therapy: AURORA study
Abstract
Aims: Heart failure (HF) is reported to be one of the major risks of bleeding events. On the other hand, HF patients frequently receive anticoagulants or antiplatelet therapy to manage various co-morbidities. However, predictors of bleeding events in patients with HF have rarely been reported. This study aimed to evaluate the predictors of bleeding events and relationship between bleeding events and HF re-hospitalizations.
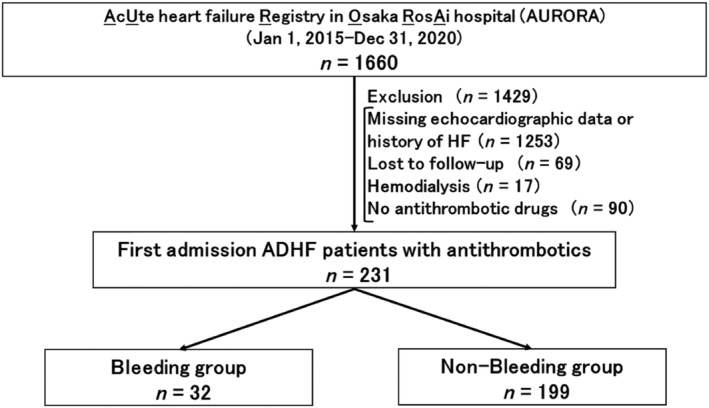
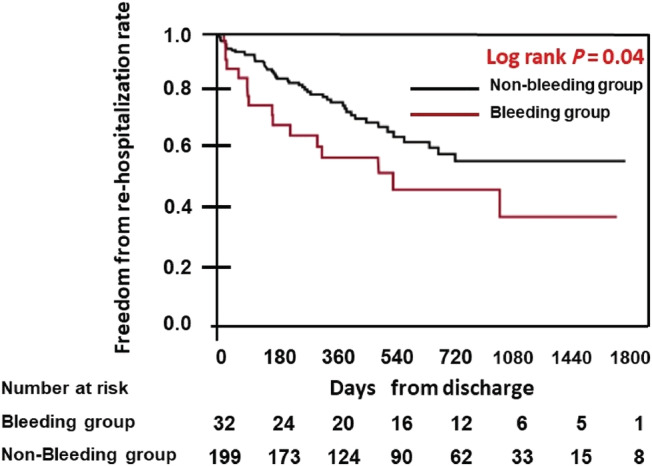
Methods and results: We included 1660 acute decompensated heart failure (ADHF) patients from the AURORA registry between January 2015 and December 2020. A total of 1429 patients were excluded because of history of HF admission, missing echocardiographic data at discharge, lost to follow-up, haemodialysis and no antithrombotic drugs. Finally, we evaluated 231 patients from AURORA registry. The bleeding events were defined as Type 2 to 5 bleeding according to the Bleeding Academic Research Consortium definition. We divided our patients into the bleeding group and non-bleeding group. We compared the baseline characteristics, medications, laboratory data, and echocardiographic data between the two groups. Median age was 78 (IQR 71-82) years old and male accounted for 59%. Approximately half of the patients had an antiplatelet therapy and 70% had an anticoagulant therapy. During a median follow-up of 651 (IQR 357-1139) days, 32 patients (13.8%) suffered from bleeding events. The major driver of the registered events was gastrointestinal bleeding (n = 21, 65.6%), and the other events were cerebral bleeding (n = 4, 12.5%), intraarticular bleeding (n = 2, 6.3%), urogenital bleeding (n = 2, 6.3%), haemorrhagic pericardial effusions (n = 1, 3.1%), subcutaneous hematomas (n = 1, 3.1%), and haemothorax (n = 1, 3.1%). There was a significantly lower haemoglobin level (P < 0.01), higher proportion of inferior vena cava (IVC) diameter ≥21 mm (P < 0.01), and higher furosemide equivalent doses per kilogram (P < 0.01) in the bleeding group than non-bleeding group. A multivariate analysis revealed an equivalent dose of furosemide per kilogram ≥0.66 mg/kg (hazard ratios (HR) of 2.64, 95% confidence interval (CI) 1.26-5.68, P = 0.01), haemoglobin ≤10.3 g/dL (HR of 2.43, 95% CI 1.14-5.03, P = 0.02), and IVC diameter ≥21 mm (HR of 2.79, 95% CI 1.16-6.29, P = 0.02) were independently associated with bleeding events. The Kaplan-Meier analysis showed that HF re-hospitalization rates were higher in the bleeding group than non-bleeding group (P = 0.04).
Conclusions: High doses of oral loop diuretics, IVC dilatation, and anaemia were predictors of bleeding events in patients hospitalized with ADHF patients. In addition, bleeding events were associated with HF re-hospitalizations.
Keywords: ADHF; Anaemia; Bleeding events; High dose loop diuretics; IVC.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Antiplatelet versus anticoagulation treatment for people with heart failure in sinus rhythm.Cochrane Database Syst Rev. 2025 Jun 11;6(6):CD003333. doi: 10.1002/14651858.CD003333.pub4. Cochrane Database Syst Rev. 2025. PMID: 40497467 Review.
-
Antiplatelet and anticoagulant agents for primary prevention of thrombosis in individuals with antiphospholipid antibodies.Cochrane Database Syst Rev. 2018 Jul 13;7(7):CD012534. doi: 10.1002/14651858.CD012534.pub2. Cochrane Database Syst Rev. 2018. PMID: 30004572 Free PMC article.
-
Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in people with antiphospholipid syndrome.Cochrane Database Syst Rev. 2017 Oct 2;10(10):CD012169. doi: 10.1002/14651858.CD012169.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Oct 12;10:CD012169. doi: 10.1002/14651858.CD012169.pub3. PMID: 28968483 Free PMC article. Updated.
-
Antiplatelet agents for the treatment of deep venous thrombosis.Cochrane Database Syst Rev. 2022 Jul 25;7(7):CD012369. doi: 10.1002/14651858.CD012369.pub2. Cochrane Database Syst Rev. 2022. PMID: 35876829 Free PMC article.
Cited by
-
Study of target INR achievement, incidence of hemorrhagic complications and affecting factors after during warfarin treatment in western area of China.Sci Rep. 2025 May 25;15(1):18200. doi: 10.1038/s41598-025-03434-5. Sci Rep. 2025. PMID: 40415097 Free PMC article.
-
Hemospray® (hemostatic powder TC-325) as monotherapy for acute gastrointestinal bleeding: a multicenter prospective study.Ann Gastroenterol. 2024 Jul-Aug;37(4):418-426. doi: 10.20524/aog.2024.0897. Epub 2024 Jun 20. Ann Gastroenterol. 2024. PMID: 38974074 Free PMC article.
-
A disproportionality analysis of adverse events associated with loop diuretics in the FDA Adverse Event Reporting System (FAERS).BMC Pharmacol Toxicol. 2025 Mar 17;26(1):63. doi: 10.1186/s40360-025-00890-7. BMC Pharmacol Toxicol. 2025. PMID: 40098168 Free PMC article.
References
-
- Natsuaki M, Morimoto T, Yamaji K, Watanabe H, Yoshikawa Y, Shiomi H, Nakagawa Y, Furukawa Y, Kadota K, Ando K, Akasaka T, Hanaoka KI, Kozuma K, Tanabe K, Morino Y, Muramatsu T, Kimura T. Prediction of thrombotic and bleeding events after percutaneous coronary intervention: CREDO‐Kyoto thrombotic and bleeding risk scores. J Am Heart Assoc. 2018; 7: e008708. - PMC - PubMed
-
- Pozzoli M, Gonzalez‐Costello J, Bayes‐Genis A, Sinagra G, Anker SD, Coats AJS, Crespo‐Leiro MG, Filippatos G, Laroche C, Maggioni AP, Mebazaa A, Piepoli MF, Tavazzi L. Prevalence of risk of thrombosis and of bleeding and antithrombotic treatment in patients with heart failure. Eur J Heart Fail. 2020; 22: 906–910. - PubMed
-
- Yoshihisa A, Kanno Y, Ichijo Y, Sato Y, Takiguchi M, Yokokawa T, Abe S, Misaka T, Sato T, Oikawa M, Kobayashi A, Yamaki T, Kunii H, Takeishi Y. Incidence and subsequent prognostic impacts of gastrointestinal bleeding in patients with heart failure. Eur J Prev Cardiol. 2020; 27: 664–666. - PubMed
-
- Nochioka K. Simplifying bleeding risk assessment in heart failure. Circ J. 2021; 86: 156, CJ‐21‐0921–157. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
