

Cardiac adipose tissue volume assessed by computed tomography is a specific and independent predictor of early mortality and critical illness in COVID-19 in type 2-diabetic patients
- PMID: 36587209
- PMCID: PMC9805370
- DOI: 10.1186/s12933-022-01722-2
Cardiac adipose tissue volume assessed by computed tomography is a specific and independent predictor of early mortality and critical illness in COVID-19 in type 2-diabetic patients
Abstract
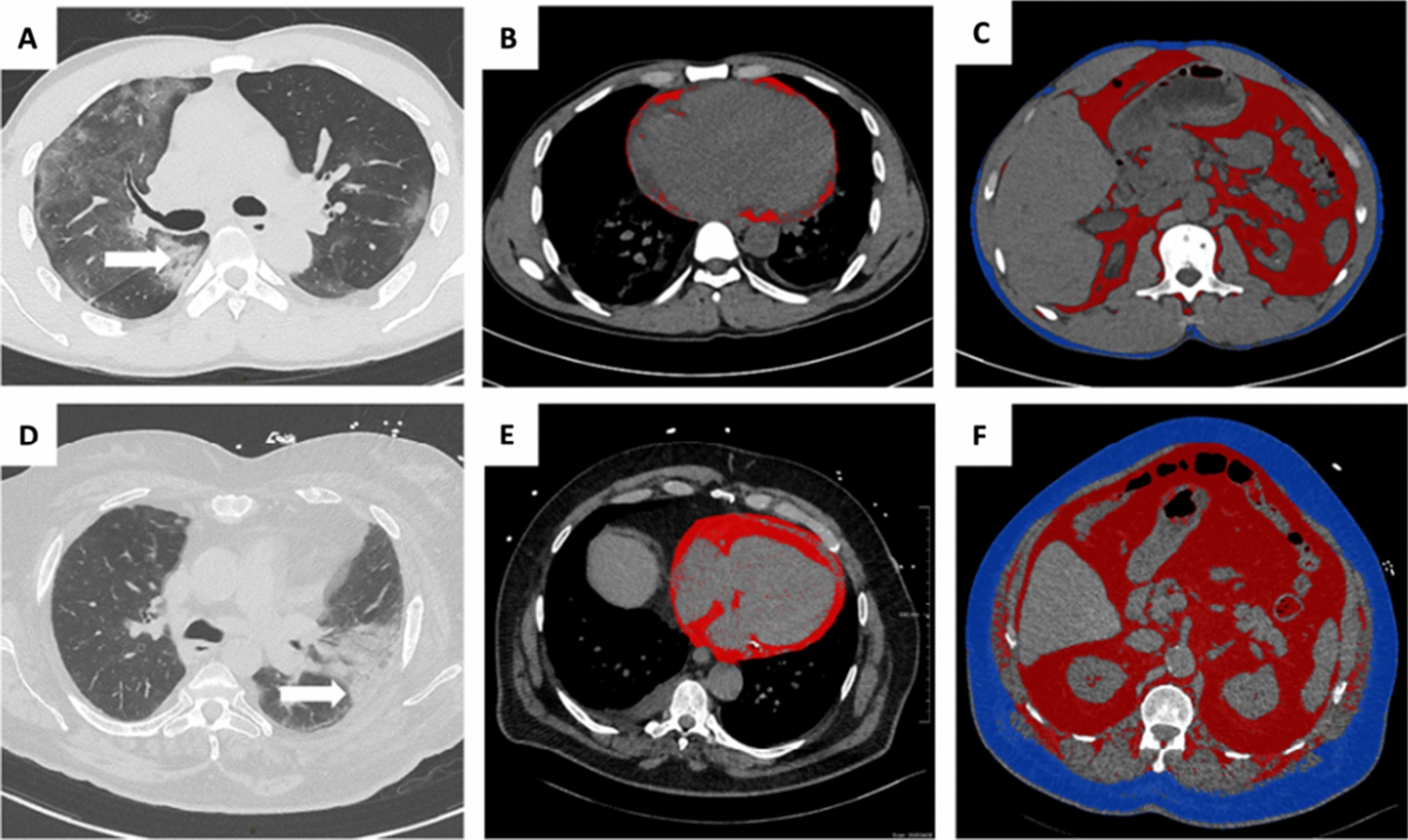
Background: Patients with type 2-diabetes mellitus (T2D), are characterized by visceral and ectopic adipose tissue expansion, leading to systemic chronic low-grade inflammation. As visceral adiposity is associated with severe COVID-19 irrespective of obesity, we aimed to evaluate and compare the predictive value for early intensive care or death of three fat depots (cardiac, visceral and subcutaneous) using computed tomography (CT) at admission for COVID-19 in consecutive patients with and without T2D.
Methods: Two hundred and two patients admitted for COVID-19 were retrospectively included between February and June 2020 and distributed in two groups: T2D or non-diabetic controls. Chest CT with cardiac (CATi), visceral (VATi) and subcutaneous adipose tissue (SATi) volume measurements were performed at admission. The primary endpoint was a composite outcome criteria including death or ICU admission at day 21 after admission. Threshold values of adipose tissue components predicting adverse outcome were determined.
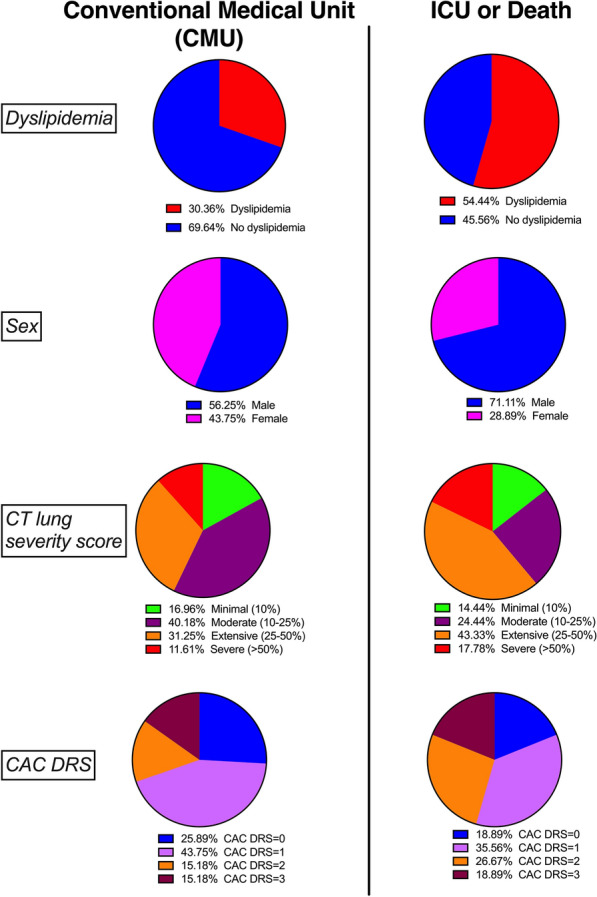
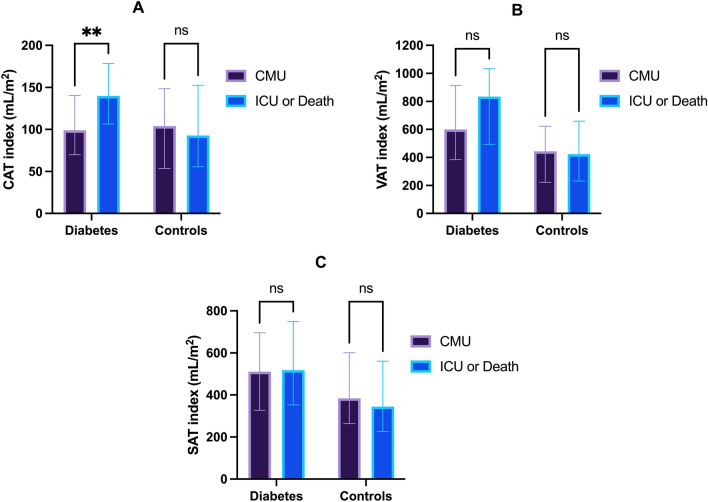
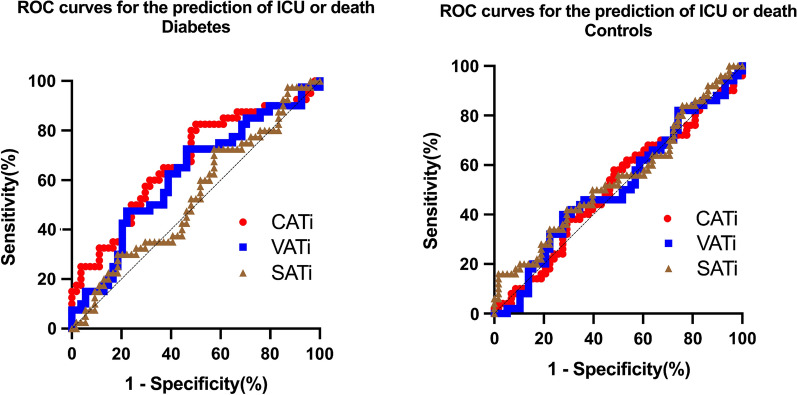
Results: One hundred and eight controls [median age: 76(IQR:59-83), 61% male, median BMI: 24(22-27)] and ninety-four T2D patients [median age: 70(IQR:61-77), 70% male, median BMI: 27(24-31)], were enrolled in this study. At day 21 after admission, 42 patients (21%) had died from COVID-19, 48 (24%) required intensive care and 112 (55%) were admitted to a conventional care unit (CMU). In T2D, CATi was associated with early death or ICU independently from age, sex, BMI, dyslipidemia, CRP and coronary calcium (CAC). (p = 0.005). Concerning T2D patients, the cut-point for CATi was > 100 mL/m2 with a sensitivity of 0.83 and a specificity of 0.50 (AUC = 0.67, p = 0.004) and an OR of 4.71 for early ICU admission or mortality (p = 0.002) in the fully adjusted model. Other adipose tissues SATi or VATi were not significantly associated with early adverse outcomes. In control patients, age and male sex (OR = 1.03, p = 0.04) were the only predictors of ICU or death.
Conclusions: Cardiac adipose tissue volume measured in CT at admission was independently predictive of early intensive care or death in T2D patients with COVID-19 but not in non-diabetics. Such automated CT measurement could be used in routine in diabetic patients presenting with moderate to severe COVID-19 illness to optimize individual management and prevent critical evolution.
Keywords: COVID-19; Cardiac adipose tissue; Computed tomography; Intensive care; Mortality; Type 2 diabetes (T2D).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests regarding this work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
