

Prospective application of the interdisciplinary bedside rounding checklist 'TEMP' is associated with reduced infections and length of hospital stay
- PMID: 36588303
- PMCID: PMC9723909
- DOI: 10.1136/bmjoq-2022-002045
Prospective application of the interdisciplinary bedside rounding checklist 'TEMP' is associated with reduced infections and length of hospital stay
Abstract
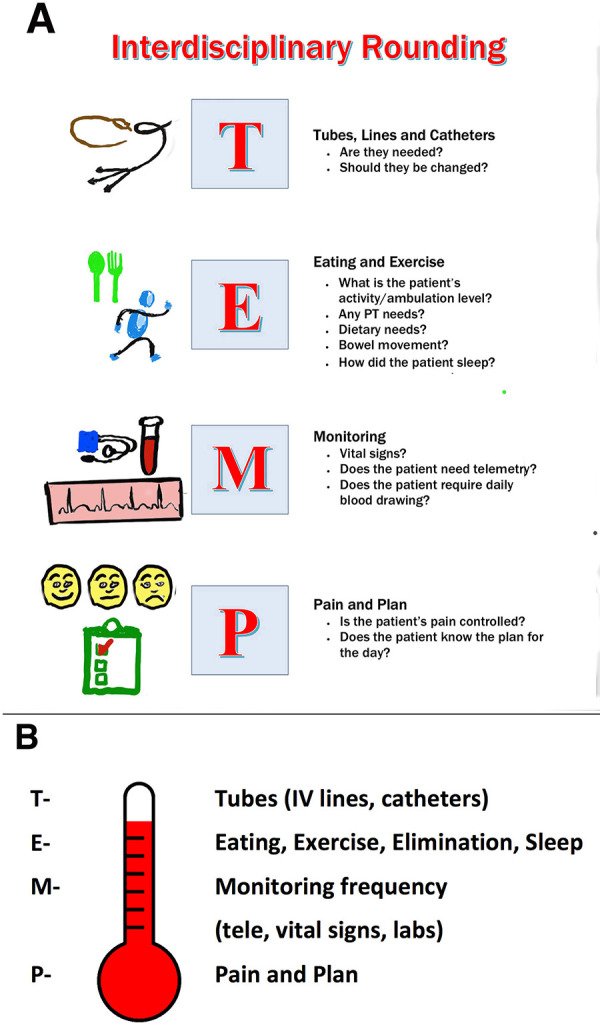
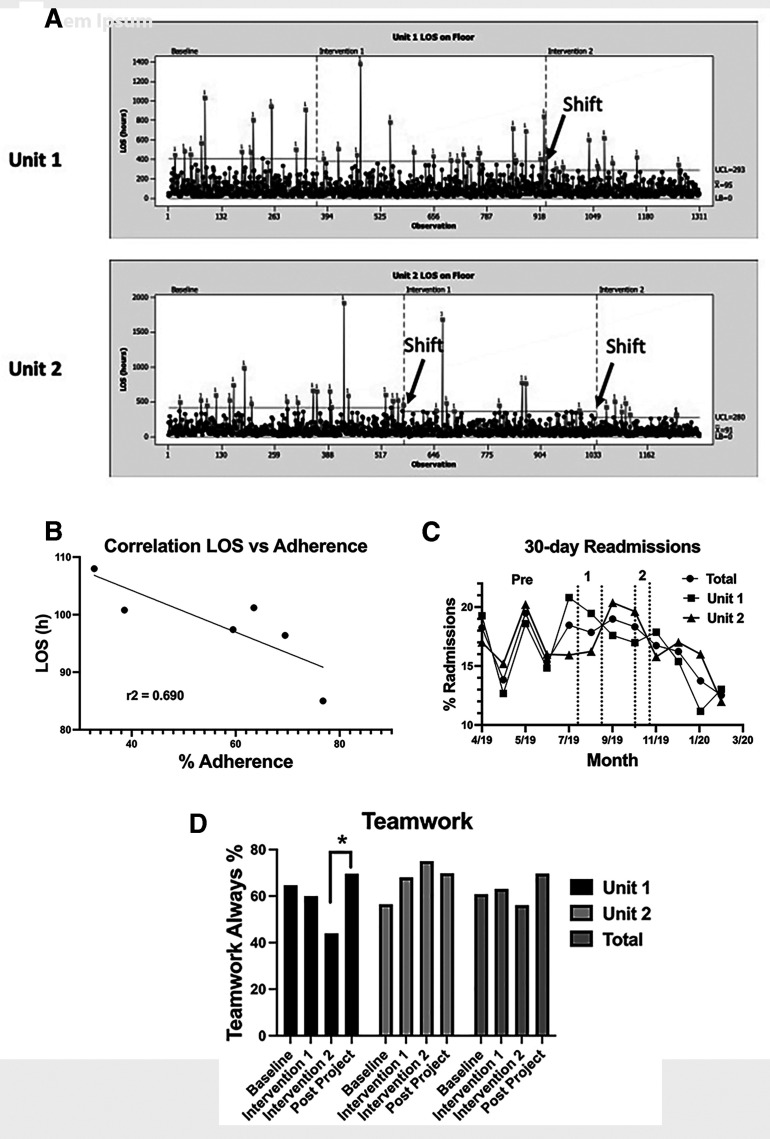
Protocols that enhance communication between nurses, physicians and patients have had a variable impact on the quality and safety of patient care. We combined standardised nursing and physician interdisciplinary bedside rounds with a mnemonic checklist to assure all key nursing care components were modified daily. The mnemonic TEMP allowed the rapid review of 11 elements. T stands for tubes assuring proper management of intravenous lines and foleys; E stands for eating, exercise, excretion and sleep encouraging a review of orders for diet, exercise, laxatives to assure regular bowel movements, and inquiry about sleep; M stands for monitoring reminding the team to review the need for telemetry and the frequency of vital sign monitoring as well as the need for daily blood tests; and P stands for pain and plans reminding the team to discuss pain medications and to review the management plan for the day with the patient and family. Faithful implementation eliminated central line-associated bloodstream infections and catheter-associated urinary tract infections and resulted in a statistically significant reduction in average hospital length of stay of 13.3 hours, one unit achieving a 23-hour reduction. Trends towards reduced 30-day readmissions (20% down to 10%-11%) were observed. One unit improved the percentage of patients who reported nurses and doctors always worked together as a team from a 56% baseline to 75%. However, the combining of both units failed to demonstrate statistically significant improvement. Psychologists well versed in implementing behavioural change were recruiting to improve adherence to our protocols. Following training physicians and nurses achieved adherence levels of over 70%. A high correlation (r2=0.69) between adherence and reductions in length of stay was observed emphasising the importance of rigorous training and monitoring of performance to bring about meaningful and reliable improvements in the efficiency and quality of patient care.
Keywords: Checklists; Communication; Continuous quality improvement; Healthcare quality improvement; Implementation science.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Increasing adherence to a standardized rounding procedure in two hospital in-patient units.J Appl Behav Anal. 2021 Sep;54(4):1514-1525. doi: 10.1002/jaba.865. Epub 2021 Jul 21. J Appl Behav Anal. 2021. PMID: 34289103
-
Implementation of a General Pediatric Clinical Rounding Checklist.Hosp Pediatr. 2019 Apr;9(4):291-299. doi: 10.1542/hpeds.2018-0150. Hosp Pediatr. 2019. PMID: 30902823
-
The Impact of Bedside Interdisciplinary Rounds on Length of Stay and Complications.J Hosp Med. 2017 Mar;12(3):137-142. doi: 10.12788/jhm.2695. J Hosp Med. 2017. PMID: 28272588 Clinical Trial.
-
The recent evolution of patient care rounds in pediatric teaching hospitals in the United States and Canada.Hosp Pract (1995). 2021 Oct;49(sup1):431-436. doi: 10.1080/21548331.2021.1977561. Epub 2021 Sep 21. Hosp Pract (1995). 2021. PMID: 34488528 Review.
-
Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Feb 18;2(2):CD012876. doi: 10.1002/14651858.CD012876.pub2. Cochrane Database Syst Rev. 2021. PMID: 33599282 Free PMC article.
Cited by
-
Quality improvement initiative to improve communication domains of patient satisfaction in a regional community hospital with Six Sigma methodology.BMJ Open Qual. 2023 Dec 30;12(4):e002306. doi: 10.1136/bmjoq-2023-002306. BMJ Open Qual. 2023. PMID: 38160018 Free PMC article.
-
Optimizing ward rounds: systematic review and meta-analysis of interventions to enhance patient safety.Br J Surg. 2025 Mar 28;112(4):znaf041. doi: 10.1093/bjs/znaf041. Br J Surg. 2025. PMID: 40202092 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources