

Procedural outcomes of chronic total occlusion percutaneous coronary interventions in patients with acute kidney injury
- PMID: 36588312
- PMCID: PMC10919567
- DOI: 10.5603/CJ.a2022.0121
Procedural outcomes of chronic total occlusion percutaneous coronary interventions in patients with acute kidney injury
Abstract
Background: The prognostic impact of contrast-associated acute kidney injury (CA-AKI) in patients undergoing chronic total occlusion (CTO) percutaneous coronary intervention (PCI) remains underestimated.
Methods: We examined 2707 consecutive procedures performed in a referral CTO center between 2015 and 2019. CA-AKI was defined as an increase in serum creatinine ≥ 0.3 mg/dL or ≥ 50% within 48 h post-PCI. Primary endpoints were in-hospital major adverse cardiac and cerebrovascular events (MACCE, composite of all-cause death, myocardial infarction, target vessel revascularization, stroke) and at one year of follow-up.
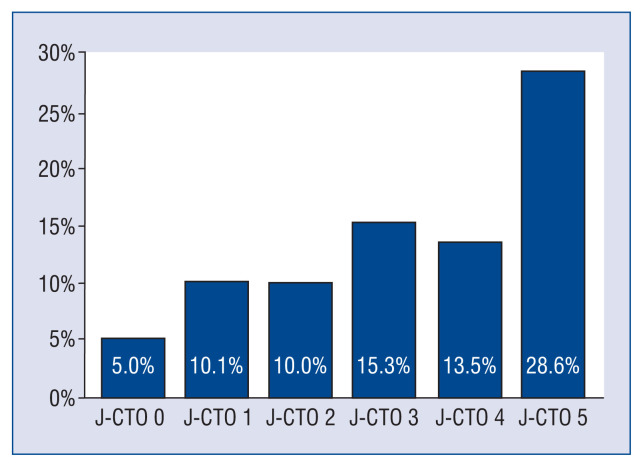
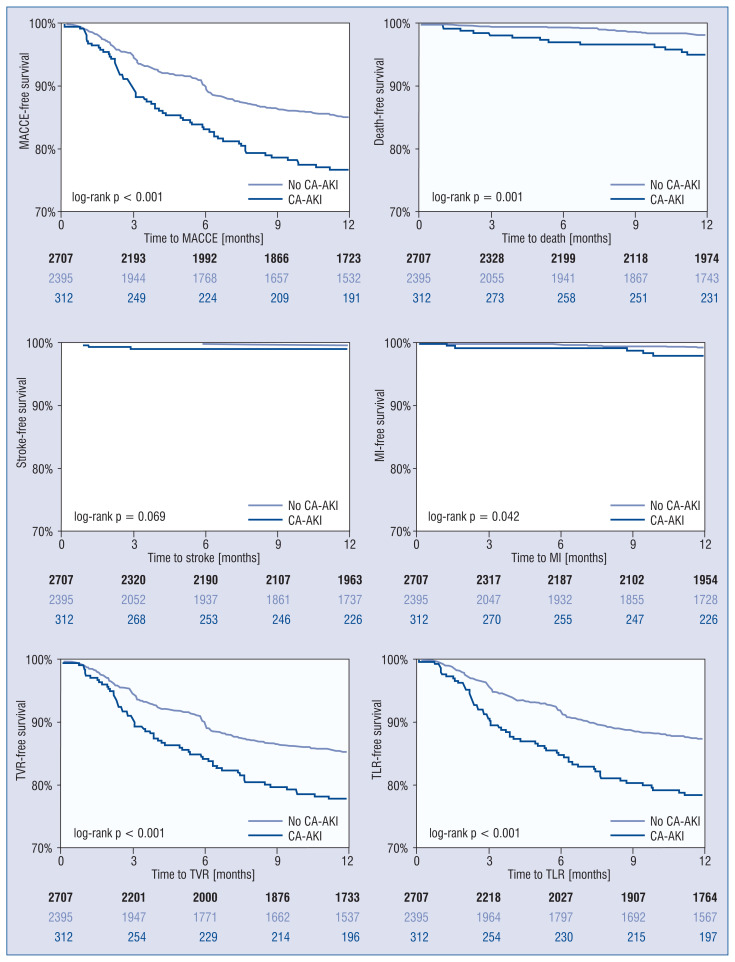
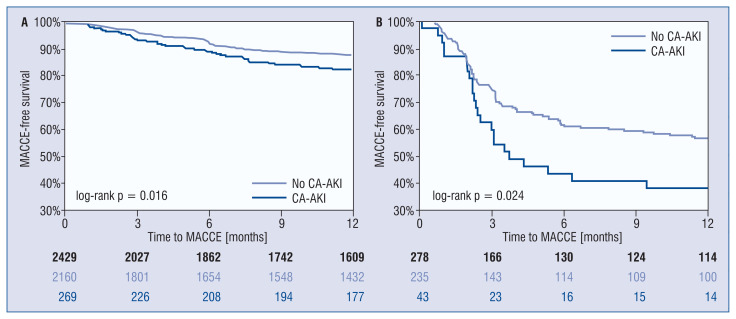
Results: The overall incidence of CA-AKI was 11.5%. Technical success was comparable (87.2% vs. 90.5%, p = 0.056) whereas procedural success was lower in the CA-AKI group (84.3% vs. 89.7%, p = 0.004). Overall in-hospital MACCE was 1.3%, and it was similar in patients with and without CA-AKI (1.6% vs. 1.3%, p = 0.655); however, the rate of pericardial tamponade requiring pericardiocentesis was significantly higher in patients with CA-AKI (2.2% vs. 0.5%, p = 0.001). In multivariate analysis, CA-AKI was not independently associated with higher risk for in-hospital MACCE (adjusted odds ratio [OR] 1.34, 95% confidence intervals [CI] 0.45-3.19, p = 0.563). At a median follow-up time of 14 months (interquartile range [IQR], 11 to 35 months), one-year MACCE was significantly higher in patients with vs. without CA-AKI (20.8% vs. 12.8%, p < 0.001), and CA-AKI increased the risk for one-year MACCE (adjusted hazard ratio [HR] 1.46, 95% CI 1.07-1.95, p = 0.017) following CTO PCI.
Conclusions: CA-AKI in patients undergoing CTO PCI occurs in approximately one out of 10 patients. Our study highlights that patients developing CA-AKI are at increased risk for long-term MACCE.
Keywords: contrast-associated acute kidney injury; outcomes; percutaneous coronary intervention.
Conflict of interest statement
Figures
References
-
- Saltzman AJ, Stone GW, Claessen BE, et al. Long-term impact of chronic kidney disease in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. JACC Cardiovasc Interv. 2011;4(9):1011–1019. doi: 10.1016/j.jcin.2011.06.012. - DOI - PubMed
-
- Latif F, Kleiman NS, Cohen DJ, et al. In-hospital and 1-year outcomes among percutaneous coronary intervention patients with chronic kidney disease in the era of drug-eluting stents: a report from the EVENT (Evaluation of Drug Eluting Stents and Ischemic Events) registry. JACC Cardiovasc Interv. 2009;2(1):37–45. doi: 10.1016/j.jcin.2008.06.012. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
